Vortex Approach
Why Vortex?
|
|
Vortex approach |
Other approaches |
|
Simple enough for real life |
Yes |
No |
|
Plan A |
Anything |
ETT only |
|
Preparation for FONA |
Early |
Late |
|
Target audience |
Anaesthetists, nurses, ambos |
Anaesthetists |
Features of Vortex:
|
|
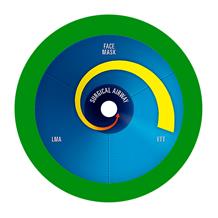
COMPONENTS: · Three lifelines 1. Bag-mask 2. LMA 3. ETT · One CICO rescue 1. FONA · Two zones: 1. Green zone (out of vortex = safe) 2. Blue zone (in vortex = spiral towards centre) 3. No grey zone! |
|
|
OPTIMISATION OF ATTEMPTS: · Max 3 attempts at each lifeline o Minimise trauma o Minimise delay · 5 Categories of optimization o Consider all o Implement only if helpful o Don’t waste time here |
|
|
SUCCESS:
·
If oxygenation ok: move to green zone · Optimise o Oxygenation o Circulation (e.g. address ignored hypotension) · Strategise 1. Keep it (proceed vs wake up) 2. Convert it (e.g. SGA -> ETT via aintree) 3. Remove and replace it (= re-enter vortex) · Mobilise: o Personnel (e.g. 2nd anaes, ENT surg) o Equipment (e.g. fibreoptic bronchoscope) o Location (e.g. to theatre from ICU) · Considerations for next strategy: o Situation (e.g. urgency of surgery) o Patient factors (e.g. aspiration risk) o Team factors (i.e. skills) o Airway factors (e.g. pathology) |
|
|
·
If oxygenation not ok: continue through
vortex · Travel in either direction · Spiral in towards CICO rescue · Can do parallel attempts (e.g. come out and bag-mask while awaiting video laryngoscope) · Must declare “Green zone” vs “Vortex” after each attempt |
|
|
CICO: · “CICO status”: o Ready: get kit o Set: open kit o Go: make cut · It’s not just about the SpO2 o High sats but tried everything -> FONA
o Low sats but haven’t tried LMA ->
LMA · Barriers to transition mindset: o ‘Flick of switch’ mentality vs ‘transitioning’ o Don’t want a reputation for a weak stomach o Airway disasters are rare o Airway disasters are insidious |
|
(not a Vortex drawing) |
CRITICAL LANGUAGE: · CPR has standardized language, e.g. o Non-shockable rhythm o Stand clear · Vortex approach offers the same o Green zone o Vortex (blue zone) o Best effort o CICO status: ready, set, go |
|
|
CLINICAL INTEGRATION: · Airway trolley should reflect vortex approach |







Feedback welcome at ketaminenightmares@gmail.com