Aortic stenosis
Disease:
|
Causes |
1. Degenerative – old 2. Congenital (bileaflet) – young 3. Rheumatic – indigenous or third world |
|
Natural history |
· Progressive deterioration · Minimal increase in gradient until 50% loss of area Annual changes: · Velocity ↑0.3m/s · AVA ↓0.1cm2 · Grad ↑4-7mmHg Time to 50% mortality: · Angina: 5y · Syncope: 3y · Dyspnoea: 2y (i.e. LV failure) Classic teaching: · High mortality if severe and symptomatic · Low mortality if severe but asymptomatic New teaching: · High mortality even if moderate (56% at 5 years) · Replace if severe / symptomatic / LV impairment (?) |
|
Secondary effects |
· Diastolic dysfunction · Systolic dysfunction · Myocardial ischaemia · Pulmonary hypertension |
|
Associations |
· Ischaemic heart disease · Other valve disease (esp if rheumatic) · Acquired vWD (shear forces -> consumption) · Mucosal and gastrointestinal angiodysplasias |
|
Differentials -Systolic murmur |
Common: · MR · HCM Uncommon: · PS · TR · VSD |
|
Treatment |
· Balloon (esp bridging) · TAVR · SAVR |
Presentation:
|
Significance |
· Poor correlation with severity of disease |
|
History |
· Angina · Syncope · Dyspnoea |
|
Examination |
Aortic stenosis: · Small volume, slow-rising pulse · Hyperdynamic, displaced apex beat · Harsh ESM at RUSB -> carotid, ± thrill Severe disease: · Weak pulse · Late-peaking murmur · Thrill · Soft S2 |
|
ECG |
· LVH (high voltage) · Strain (ST depression + T wave inversion) |
Echo:
|
Suggestive |
· PLAx and PSAx views · Thickened and restricted · Abnormal number of leaflets |
|
Diagnostic |
PSAX view: · Number of leaflets · Appearance of restriction · Presence of regurgitation PLAX view: · Velocity: o CWD through LVOT · Mean gradient: o Simplified Bernoulli equation (∆P = 4v2) o Usually greater than LHC pull-back gradient · Valve area: o Conservation of mass o VTILVOT x areaLVOT = VTIAV x areaAV · Velocity ratio = dimensionless index o LVOT VTI : AV VTI o <0.25 indicates severe disease o Important in low flow, low gradient AS |
|
Complications |
· LVH: ↑wall thickness · LA enlargement: ↑diameter · Diastolic dysfunction: A4C view – abnormal E/A, ↑E/E’ · Systolic dysfx: PLAx and PSAx views – reduced motion · PHTN: A4C view – CWD at TR jet > 2.8m/s |
Grading:
|
|
Mild |
Moderate |
Severe |
|
Velocity |
2-3 |
3-4 |
>4 |
|
Mean gradient |
5-20 |
20-40 |
>40 |
|
Valve area |
1.5-2.5 |
1-1.5 |
<1 |
|
Dimensionless index |
0.5-1 |
0.25-0.5 |
<0.25 |
Anaesthesia issues:
|
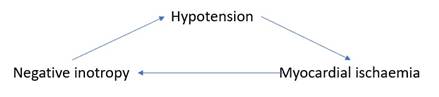
Death spiral |
|
|
Ischaemia risk |
· ↑Demand: hypertrophy + pressure work · ↓Supply: if hypotension (common in anaesthesia) |
|
Low cardiac output |
· Dependent on SVR for mAP |
|
Fixed cardiac output |
· Dependent on HR for CO |
|
Diastolic dysfunction |
· Dependent on preload, but also risk of pulmonary congestion · Dependent on sinus rhythm |
|
Pulmonary HTN |
· See other document · Maintain coronary perfusion · Minimise afterload i.e. PVR |
Anaesthesia management:
|
Goals |
· Full: euvolaemia for preload · Slow: normal HR for filling time, sinus rhythm for atrial kick · Tight: maintain SVR hence mAP hence coronary perfusion |
|
Access |
· Arterial line pre-induction · Large IV + pumpset · ±CVC if impaired systolic function |
|
Monitoring |
· Standard · 5 lead ECG · Arterial line · PPV |
|
Induction drugs |
· Don’t do a spinal · CSL 250mL bolus · Metaraminol infusion 10mg/h · Fentanyl 5mcg/kg · Propofol 1-2mg/kg very slowly until LOC · Rocuronium 0.6mg/kg at LOC |
Feedback welcome at ketaminenightmares@gmail.com