Congenital heart disease
List:
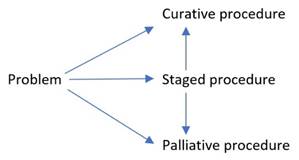
· Clinical pathways
· Left to right shunt
· Right to left shunt (TOF)
· Univentricular heart (HLHS)
· Fontan surgery
· Fontan circulation
Pathways for congenital heart disease:
Left to right shunt:
|
Problem: |
· Not perfusing the tissues = heart failure |
|
Examples |
· ASD, VSD · AP window · Truncus arteriosus |
|
Goals |
↑PVR: · Physical: ↑PEEP (7-8) · Physiological: ↓SaO2 (90%), ↑PaCO2 (45-50) ↓SVR: · Occurs by default under GA |
|
Causes of hypoxaemia |
· Airway: ETT endobronchial, dislodged, occluded · Breathing: de-recruitment · Circulation: rarely |
Right to left shunt:
|
Problem: |
· Not oxygenating the blood = hypoxaemia |
|
Examples |
· Tetralogy of Fallot · Transposition of the great arteries |
|
Goals |
↑SVR: · Physical: flex the hips · Pharmacological: alpha agonist, minimize anaesthetic ↓PVR: · Physical: lung volume at FRC, ↓airway pressure · Physiological: ↑PaO2, ↓↔PaCO2, ↔temp, ↔pH · Pharm: anaesthetics, vasodilators |
|
Cause of hypoxaemia |
· Airway: as before · Breathing: as before
·
Circulation:
often |
Tetralogy of Fallot:
|
Problem |
· Not oxygenating the blood = hypoxaemia · RVOTO |
|
Features |
· RVOT obstruction -> RVH · AVSD with aorta overriding it |
|
Goals |
↑SVR: · Physical: flex the hips · Pharmacological: alpha agonist ↓PVR: · Physical: ↓PEEP · Physiological: ↑PaO2, ↓PaCO2 · Pharm: anaesthetics, vasodilators Prevent RVOTO: (like right-sided HOCM) · Full · Tight · Slow |
Hypoplastic left heart syndrome:
|
Problem |
· Only one pump for both pulmonary and systemic circulations |
|
Severity |
· Patency of ductus (if not, then dead) · Patency of foramen ovale (if not, then dead) · Function of remaining ventricle · Balance of Qp (oxygenation of blood) and Qs (perfusion of tissues) |
|
Management |
· Deliver near a tertiary children’s hospital Keep the ductus arteriosus open: · PGE1 for DA (side effects: apnoea, ↓plt) Goldilocks flow allocation: · PVR high enough to allow systemic flow (incl heart and brain) · PVR low enough to allow pulmonary flow · Ideal SaO2 85% · May require ETT + IPPV · May require FiO2 <0.21 Strong ventricle: · RV is not designed for high afterload · Low-normal SVR · ±Inotrope |
Surgery for hypoplastic left heart syndrome
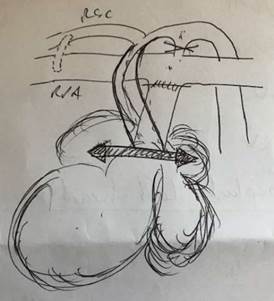
Stage 1: Norwood procedure (1-3 days)
|
Picture |
|
|
Aims |
· Supply both lungs and body · Allow the child to grow |
|
Operation |
· Atrial septectomy · Fashion the main PA into an aorta · Close the ductus arteriosus · Create a new systemic-to-pulmonary shunt o e.g. Blalock-Taussig shunt: right subclavian to right PA o Small hole to avoid stealing too much |
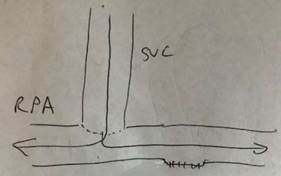
Stage 2: Bi-directional cavo-pulmonary shunt (2-6 months)
|
Picture |
|
|
Aims |
· Partially separate the systemic and pulmonary circulations o Improve cyanosis a bit o Offload the ventricle a bit |
|
Operation |
· Create a systemic-venous-to-pulmonary-arterial shunt o i.e. SVC to right pulmonary artery o Big hole is ok now because venous pressure is lower · Close the systemic-arterial-to-pulmonary-arterial shunt |
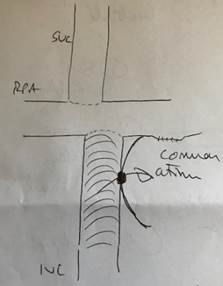
Stage 3: Fontan procedure (2-6 years)
|
Picture |
|
|
Aims |
· Separate the systemic and pulmonary circulations completely · Hence improve cyanosis even more (SaO2 ~90% is the new normal) · Hence offload the ventricle even more |
|
Operations |
· Complete the systemic-venous-to-pulmonary-arterial shunt o i.e. IVC to right pulmonary artery via Dacron graft · Create a pop-off valve o Communication between the Dacron graft the common atrium |
|
Problems |
· Many complications · Causes: incl high CVP, disrupted lymphatics · e.g. chylothorax, ascites, oedema, protein-losing enteropathy |
Fontan circulation:
|
Problem: |
· No accessory pump to fill the main pump |
|
Goal: |
· Maintain venous return (“trans-pulmonary gradient”) |
|
↑Pressure1 |
i.e. CVP (~10-12mmHg) · Euvolaemia · Jack-knife position |
|
↓Resistance |
i.e. PVR
Physiology: · ↑PaO2 · ↓PaCO2 · ↔pH · ↔Temp Pharmacology: · General anaesthetics · Vasodilators · Avoid histaminergic drugs (atrac, sux, morph) Ventilation: · ↔Lung volume · ↔Airway pressure · Spont vent if possible · ↓PEEP · ↑Expiratory time |
|
↓Pressure2 |
i.e. atrial pressure ~7-8mmHg · Sinus rhythm · ↔Contractility · ↓Afterload · A-V valve functioning |
Other Fontan issues:
· Complications of ↑CVP
· Thromboembolism
· Infections
· Valvular regurgitation
Feedback welcome at ketaminenightmares@gmail.com