TAVI
Pre-op issues:
|
Assessment |
· Aortic stenosis · Associated cardiac disease (e.g. failure) · Comorbidities |
|
Planning |
· MDT · Nothing vs TAVI vs SAVR |
|
Optimisation |
· Medication · Fluid |
Intra-op issues:
General:
|
Remote environment |
· Prepare for airway difficulty · Prepare for vascular injury · Prepare for arrest |
|
Sedation vs GA |
Sedation benefits: · Avoid haemodynamic insult of GA · Rapid V-pacing is well tolerated · Shorter procedure and hospital stay
GA benefits: · Can do TOE: detect paravalvular leak · Prepared for vascular disaster
Sedation pre-requisites: · Can lie flat · Can lie still · Can co-operative · Can keep airway patent (i.e. beware OSA + sedation) |
TAVI:
|
Vascular disaster |
· Cardiac surgeon + perfusionist + gear on-site · Group and hold · Consent for blood transfusion |
|
Valve deployment / balloon dilatation |
· Need rapid ventricular pacing + apnoea · Prepare: FiO2 100%, SBP 120mmHg |
Aortic stenosis:
|
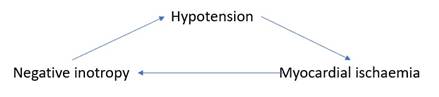
Death spiral |
|
|
Goals |
· Full: euvolaemia for preload · Slow: normal HR for filling time, sinus rhythm for atrial kick · Tight: maintain SVR hence mAP hence coronary perfusion |
|
Ischaemia risk |
· ↑Demand: hypertrophy + pressure work · ↓Supply: if hypotension (common in anaesthesia) |
|
Low cardiac output |
· Dependent on SVR for mAP |
|
Fixed cardiac output |
· Dependent on HR for CO |
|
Diastolic dysfunction |
· Dependent on preload, but also risk of pulmonary congestion · Dependent on sinus rhythm |
|
Pulmonary HTN |
· See other document · Maintain coronary perfusion · Minimise afterload i.e. PVR |
Complications:
· Bleeding
· Stroke
· Paravalvular regurgitation
· AV block
· Arrhythmias
· Annular rupture
· Myocardial injury
· Tamponade
· Mitral valve damage
· Hypotension
· Dynamic LVOTO
· Death
Feedback welcome at ketaminenightmares@gmail.com