Miscellaneous:
|
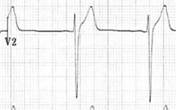
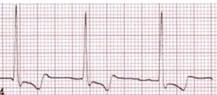
Benign early repolarization |
· Normal finding in young, healthy patients · a.k.a. high take off, J point elevation · Mainly in V2-5 · Concave ST elevation + notched J point + asymmetrical T wave · Absence of reciprocal ST depression elsewhere
|
|
HCM |
· LVH criteria · Septal pattern: dagger-like Q waves laterally and inferiorly
· Apical pattern; giant inverted T waves praecordially
|
|
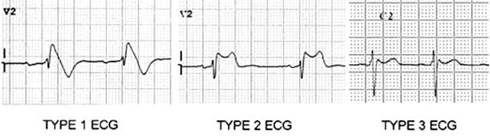
Brugada |
· Na+ channelopathy · ST elevation in V1-3 · Type 1: coved shape · Type 2: saddle shape · Type 3: either but <2mm
|
|
WPW |
· Accessory pathway between atria and ventricle (Bundle of Kent) · Resting: ↓PR interval, ↑QRS, slurred upstroke (δ) in V1, abnormal T wave
·
Pre-excited AF: if AF and VT had a baby o NO: give node blocking drugs (adenosine, b-blocker, CCB) o YES: cardioversion, flecainide (normal LV), amiodarone (abnormal LV) · Orthodromic SVT: o Looks like vanilla SVT o Treated like vanilla SVT · Antidromic SVT: o Looks like VT o Treated like VT |
|
Lung disease |
Findings can include: · Right axis deviation · Atrial arrhythmias · P pulmonale · RBBB · RVH · RV strain pattern |
|
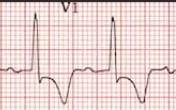
RV strain |
· ST depression, T wave inversion V1-4 and inferiorly
|
|
HyperK |
1. Tall, tented T waves 2. Small or absent P waves 3. Widened PR 4. Widened QRS 5. Sine wave 6. Asystole |
|
HypoK |
· Repolarisation: ST depression, T wave flattening, ±U wave · Conduction: AV block, prolonged QT · Ectopy: PAC, PVC, VT if severe |
|
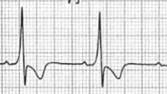
Digoxin effect |
· Reverse tick · Especially lateral leads · Can be widespread · N.B. does not indicate toxicity (that’s VT or VF)
|
|
LAST |
· Conduction delay (as if ‘pulled apart’)
· Tachyarryhthmias (VT, VF) |