Tachyarrhythmias:
|
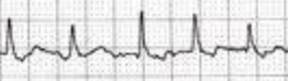
AF |
· Wandering baseline · Irregularly irregular QRS · Variable amplitude of QRS (∝ ventricular filling)
|
|
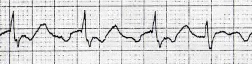
AFL |
·
Classic: sawtooth baseline ·
Real life: hidden in ST segment · Often 300 per minute · Often fixed conduction interval e.g. 2:1, 3:1 · Circuit goes up and down -> best seen in inferior leads |
|
SVT |
AVNRT: · i.e. SVT · Narrow complex and regular · Rate 150-200 · May or may not see P waves (retrograde and/or swallowed up) · Rx: Valsalva + legs up, adenosine
AVRT: · Abnormal pathway between atria and ventricles · e.g. WPW (see “Miscellaneous”) · Orthodromic: narrow QRS (treated like vanilla SVT anyway) · Antidromic: wide QRS (look out!) |
|
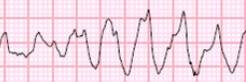
VT |
· Monomorphic
· Polymorphic
o Torsades: QRS complexes ‘twist’ around the isoelectric line
|
|
Broad complex tachycardia |
DDx: · VT (best to assume) · SVT with o BBB o Accessory pathway o Certain anti-arrhythmics o Profound hyperkalaemia Problem: · The above look alike · Some drugs safe, others lethal · Call cardiology for help Factors suggesting VT: (Brugada criteria) · Doesn’t look like a BBB · Axis in no-man’s land · Very broad complexes · AV dissociation · Capture beats (occasional normal-looking QRS) · Fusion beats (concurrent VT beat and sinus beat -> weird QRS) |
|
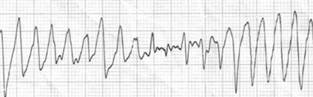
VF |
· Why are you doing a 12 lead? |