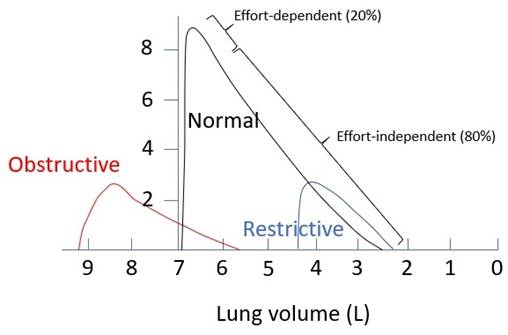
2017A11 Draw an expiratory
flow-volume curve obtained from a maximal expiratory effort after a
vital capacity breath,
for a person with a) normal lungs b) restrictive lung disease b)
obstructive lung disease (10 marks).
Explain how and why these curves (and the derived parameters) are
different for each disease state (15 marks).
List:
· Diagramme
· Relevant physiology
· Normal flow-volume curve
· Obstructive pathophysiology
· Restrictive pathophysiology
Diagramme:
Relevant physiology:
|
Flow determinants |
· Ohm’s law: Expiratory flow rate (Q) = (PAlv-Patm)/airway resistance · Normal values o PAlv: 38cmH2O o Patm: 0cmH2O by definition o AWR: 2cmH2O/L/s · Factors ↑Q: ↑PAlv, ↓Patm, ↓AWR |
|
Resistance |
· Laminar flow (small airways): R = (8 x length x viscosity) / (π x radius4) · Turbulent flow (large airways): (P1-P2) ∝ (length x density) / radius5 · Factors ↓AWR o ↑Radius (most important since raised to power 4 or 5) o ↓Viscosity (e.g. temp) o ↓Density (e.g. heliox cf. air) o ↓Length (not under control) |
|
Dynamic airways compression (DAC) |
· Pressure drop occurs between alveolus and mouth due to airway resistance · Where airway pressure = intrapleural pressure, unsupported airways collapse o i.e. equal pressure point (EPP) o Starling resistor mechanism; P2 = PIP not Patm o Cartilage absent after generation 11 |
Normal flow-volume curve:
|
TLC |
· Lung volume after maximal inspiratory effort · Note unable to measure with flow-volume curve |
|
Upward slope |
· Effort-dependent · Radial traction distends airways |
|
Max PEFR |
· Occurs at beginning of forced expiration. o Highest lung elastic recoil o Highest airway radius o ? High expiratory muscle mechanical advantage · Reflects larger airway function · Mainly effort-dependent · Limited by onset of DAC |
|
Linear decline |
· Mainly effort-independent, especially FEF25-75% · Decline due to increasing DAC as lung volume and airway radii fall · Mostly effort independent · Reflects smaller airway function |
|
RV |
· Maximal expiration · Limited by small airway closure · Note unable to measure with flow-volume curve |
|
FVC |
· = TLC - RV |
Obstructive pathophysiology:
|
Example |
· Asthma, COPD |
|
?TLC |
· COPD with emphysema: ↓elastic recoil · (? Asthma: gas trapping – not clear to me if this is true) |
|
↓Upward slope |
· Cause: ↓airway radius |
|
↓PEFR |
· ↓Airway radius · Earlier and exaggerated DAC, distal migration of EPP |
|
Linear decline |
· Scooped out appearance, ↓FEF25-75% o Earlier and exaggerated DAC, distal migration of EPP o (if emphysema: ↓radial traction, ↓lung recoil) · Changes ∝ severity |
|
↑RV |
· ↓Airway radius -> earlier airway closure · (if emphysema: ↓lung recoil, earlier airway closure) |
|
↓FVC |
· ∆RV > ∆TLC |
Restrictive pathophysiology:
|
Example |
· Pulmonary fibrosis |
|
↓TLC |
· ↓Lung compliance |
|
↔↑ Upward slope |
· ↑Lung recoil |
|
↔↓Max PEFR |
· (affected in severe disease) · ↓Lung compliance |
|
Linear decline |
· ↔↑Slope, especially at end-expiration o ↑lung recoil -> ↑ transpulmonary pressure o Stiff, less collapsible tissue |
|
↓RV |
· ↑Lung recoil -> airway closure at lower lung volume |
|
↓FVC |
· ∆TLC > ∆RV |
Feedback welcome at ketaminenightmares@gmail.com