2019A15 Explain the reasons why a pulse oximeter may give incorrect readings.
List:
· Pulse oximetry principles: device, physical basis, how it works (keep it brief)
· Sources of error: intrinsic, probe, patient
Pulse oximetry:
|
Components |
· Probe on the finger, nose, ear · Two monochromatic LEDs on one side, rapid on and off · Photodetector on the other side · Cable to processor/display |
|
Physical basis |
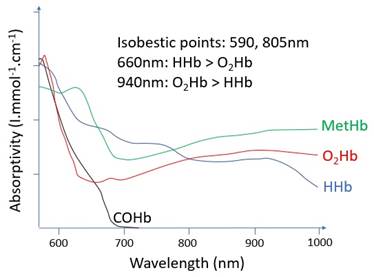
(1)Beer-Lambert principle: I = I0e-ax · Aborption ∝ concentration of the absorbing substance in the medium (Beer’s law) · Absorption ∝ distance travelled through the medium (Lambert’s law) · Describes the basis for, but not the functioning of, the pulse oximeter (2)Known absorption spectra: · 940nm: HbO2 > HHb · 660nm: HbO2 < HHb
|
|
How it works |
(1)Pulsatile signal isolated · Exclude venous and tissue absorption (2)Ratio of absorbances calculated · Ratio = (pulsatile660 / non-pulsatile660) / (pulsatile940 / non-pulsatile940) (3)Ratio correlated with SaO2 derived from experiments · R 0.4 -> 100% · R 1 -> 85% · R 2 -> 50% |
Causes of inaccuracy:
|
Intrinsic |
· Low extreme of range o 70-100% ±2 o 50-70% ±3 o <50% inaccurate · Lag time for signal: signal averaged over 10-20 seconds · Lag time for problem: o e.g. airway obstruction -> delay between problem and detection · Unable to discern dyshaemoglobins due to number of LEDs o HbCO: tends toward 96% o MetHb: tends towards 85% · May be inaccurate in arrhythmias (variation in pulse amplitude) |
|
Probe |
· Physical interference: o Excessive movement o Ambient light o Nail varnish · Electrical interference: especially diathermy |
|
Patient |
· Inadequate signal: o ↓Cardiac output o Vasoconstriction o Hypothermia · Venous pulsation confused for arterial: o ↑CVP o Severe TR |