2020B13 Describe the principles (50%) and sources of error (50%) in the measurement of arterial blood pressure using an invasive arterial line and transducer.
List:
· Diagramme
· Components
· Function
· Calibration
· Sources of error
Diagramme:
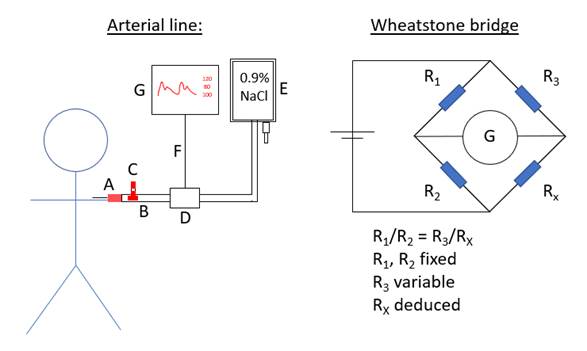
Components:
|
A |
Catheter |
20 or 22 gauge Short, wide (20g or 22g), stiff Clot-resistant, kink resistant material e.g. FEP polymer |
|
B |
Tubing |
Short (<1.2m), wide (lumen >1.5mm), stiff tubing Low density fluid (saline) |
|
C |
Sampling port |
Sampling port and three-way tap |
|
D |
Transducer |
Infusion at 3mL/h Rapid flush lever for a) clearing the catheter b) test for damping |
|
E |
Reservoir |
0.9% NaCl at 300mmHg |
|
F |
Electrical cable |
|
|
G |
Processor Display |
May include other functions including pulse pressure variation, pulse contour analysis |
Function:
|
Oscillation |
· Oscillations in arterial pressure transmitted to saline column · Column displaces transducer’s diaphragm and strain gauge |
|
Transduction |
· Stretch of strain gauge increases electrical resistance · ±Multiple strain gauges in Wheatstone bridge for accuracy · Electrical signal transmitted to processing unit |
|
Processing |
· Signal filtered + amplified · Signal broken down into component sine waves (Fourier analysis) · Waveform constructed using fundamental freq + several harmonics · Read-outs calculated |
|
Display |
· SBP, DBP, mAP and waveform displayed on the monitor · +/- Pulse pressure variation, pulse contour analysis |
Calibration:
i.e. static accuracy
|
Zero point |
· Relative to atmospheric pressure · “Off to patient, open to air” |
|
Height |
· Raise transducer against a standard · 7.4mmHg per 10cm |
|
Time |
· Observe steadiness at zero across time |
Sources of error:
|
Static inaccuracy: |
|
|
- Zero |
Failure to calibrate: · Unpredictable. False ↑ or ↓ |
|
- Height |
Failure of target selection: · If supine: phlebostatic axis (4th intercostal space, mid-axillary line) · If beach chair: brainstem (external acoustic meatus) Failure to adjust with patient movement: · Transducer too high: BP falsely low · Transducer too low: BP falsely high
Risk: overtreat ↑BP or undertreat ↓BP -> organ ischaemia |
|
- Time |
· Natural drift of strain gauge. False ↑ or ↓ · Equipment dysfunction. False ↑ or ↓ |
|
Dynamic inaccuracy: |
|
|
- Resonance |
= exaggeration of oscillatory amplitude if system stimulated at a close multiple of natural frequency (FN) ->>False ↑SBP, ↓DBP, ↔ mAP
Avoided if FN > 10x F0 (heart rate): · ↑potential energy: stiff tubing and diaphragm · ↓kinetic energy: short, wide, stiff tubing and cannula; and low density fluid |
|
- Damping |
= minimisation of oscillatory amplitude through viscosity and friction ->> Overdamped:
False ↓SBP, ↑DBP, ↔ mAP
Optimised if damping coefficient 0.64 ·
Intact cannula, no kink/blood/clot/bubble · Optimal cannula and tubing design
|
N.B. modern systems are underdamped, but natural frequency is sufficiently high to prevent resonance
Feedback welcome at ketaminenightmares@gmail.com