2000A15 Describe the effects of opioids on the respiratory system.
List:
· Respiratory depression
· Airway reflex depression
· Other
Respiratory depression:
|
Mechanism |
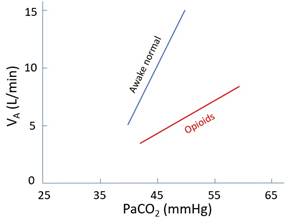
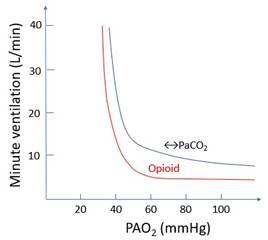
· MOP, DOP in resp centre in dorsal medulla · Much less effect on chemoreceptors? · ↓RR more than ↓VT; risk of apnoea · If also sedated: risk of airway obstruction -> death · ↓↓Response to ↑PaCO2 (↑apnoeic threshold and ↓gain; dose-dependent) · ↓Response to ↓PaO2 (dose-dependent)
|
|
Therapeutic index |
· Morphine 70 · Fentanyl 400 · Sufentanil 27,000 · Remifentanil 33,000 · (Note effects begin in the analgesic range (e.g. fentanyl 2-5ng/mL)) |
|
Risk factors |
· Other drugs: o Benzodiazepines: synergistic depression o Residual volatile anaesthetic -> ↓↓ responsiveness to ↓PaO2 · Patient: o Neonate: immature respiratory centre, immature BBB -> ↑morphine effect o Elderly: ↑PD sensitivity o Sleep -> ↓responsiveness to ↓PaO2 and ↑PaCO2 · Pathology: o Hypothermia -> ↑sensitivity o Denervated carotid body -> no response to ↓PaO2 o Desensitised respiratory centre (OSA, OHS) |
|
Protective factors |
· Pain · Chronic opioid use (note tolerance varies considerably) |
|
Timing |
· Drug: o ↑Lipid solubility, ↑%unionised -> faster peak effect (e.g alfentanil) o ↓Lipid solubility, ↓% unionised -> slower peak effect (e.g. morphine) o Partial agonist -> ↓risk respiratory depression (e.g. buprenorphine) · Route: o IV -> highest peak effect o IM/SC -> lower peak effect but risk of dose stacking if low skin/muscle blood flow o Intrathecal: peak effect fentanyl 30mins (systemic absorption), morphine 6-12 hours (CSF circulation) |
Airway reflex depression:
|
Receptor |
· MOP |
|
Location |
· Medulla |
|
Effects |
· ↑ETT tolerance · ↓Cough, ↓laryngospasm · ↓Risk laryngospasm |
|
Use |
(particularly remifentanil) · Intubation without paralysis (e.g. neuromuscular disorder, large intracranial aneurysm) · Extubation without coughing (e.g. neurosurgery) |
Other:
|
Chest wall rigidity |
· Associated with remifentanil boluses · May herald uncconsciousness · Cause: MOP on GABA-ergic neurons in basal ganglia · Problem: unable to ventilate · Rx: paralyse |
|
Bronchospasm |
· Morphine -> MOP on mast cells -> histamine release |
|
Ciliary dysmotility |
· ? Mechanism |
|
Antisialogogue |
· Especially pethidine: muscarinic ACh receptor antagonist |
Feedback welcome at ketaminenightmares@gmail.com