2013B12 Explain
how the differences in pharmacokinetics of alfentanil and fentanyl can
influence the way
they are administered intravenously.
List:
· Distribution
· Elimination
· CSHT
Distribution:
|
|
Fentanyl |
Alfentanil |
Implication |
|
-Lipid solubility |
600x |
90x |
May partly account for VDSS FENT >> ALF |
|
-pKa (both weak bases) |
8.4 |
6.5 |
|
|
-% unionised at pH 7.4 |
9% |
89% |
Main reason for ALF’s short time to peak effect (TTPE) Offsets lower lipid solubility |
|
-%Plasma protein bound |
83% |
90% |
|
|
-VDC (L/kg) |
0.2 |
? |
|
|
-VDSS (L/kg) |
4 |
0.6L/kg |
FENT faster offset if short infusion ALF faster offset if long infusion |
|
-t1/2ke0 (mins) |
6.9 |
0.9 |
ALF: high % unionised offsets low LS |
|
-t1/2α (mins) |
1 fast, 18 slow |
1 fast, 14 slow |
Both rapid offset after single bolus |
Elimination:
|
|
Fentanyl |
Alfentanil |
Implication |
|
Metabolism |
Liver. CYP3A4 > other |
Liver. CYP3A4,5 |
|
|
Metabolites |
Inactive Norfentanyl > other |
Inactive Noralfentanil > other |
Both safe in renal failure |
|
Cl (mL/kg/min) |
13 |
6 |
|
|
t1/2β (mins) |
190-475 |
70? 100? |
Note ALF ↓Clearance but ↓↓VDSS t1/2β = VD/Cl x loge2 Hence offset after long infusion ALF >> FENT |
|
Excretion |
Metabolites -> urine |
Metabolites -> urine |
|
Time course:
|
|
Fentanyl |
Alfentanil |
Implication |
|
-Onset (time to 80%) (mins) |
3 |
1.2 |
Alfentanil for brief intense stimulation e.g. laryngoscopy e.g. lancing peri-anal abscess. Fentanyl for medium to long duration surgery e.g. lap cholecystectomy e.g. CABG |
|
-TTPE (mins) |
5 |
1.8 |
|
|
-Duration (mins) |
10 (highly dose-dependent) |
4 |
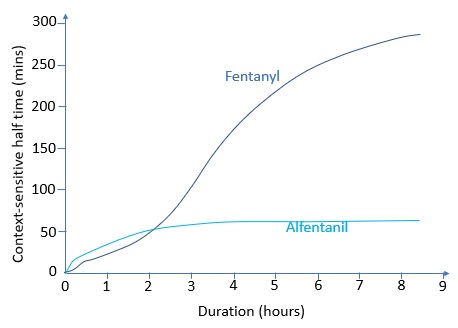
Context sensitive half time:
|
Graph |
|
|
Difference |
· <2 hours: fentanyl’s CSHT is shorter o Large VDSS, moderate clearance rate o Suited to bolus or short infusion o Can administer large bolus for prolonged effect (e.g. CP bypass) · >2 hours: alfentanil’s CSHT is shorter o Very low VDSS, low clearance o Suited to bolus and/or variable length infusion (?) |