2021A10 Describe
the clinical effects of non-steroidal anti-inflammatory drugs
including mechanisms through which they exert these effects.
List:
· Classification and examples
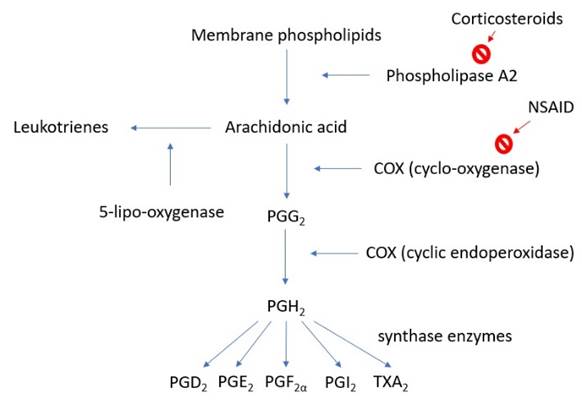
· Arachidonic acid pathway
· Prostaglanding receptors
· The big 3 effects
· Organ system effects
· COX-2 selective
NSAID classification: (examiner request)
|
Non-selective irreversible |
· Salicylates: aspirin |
|
Non-selective reversible |
· Propioinic acids (e.g. ibuprofen, naproxen) · Phenylacetic acid derivative (e.g. diclofenac) · Indoles (e.g. indomethacin) · Enolic acid derivatives (e.g. meloxicam) · (many others) |
|
COX-2 selective |
· Celecoxib · Parecoxib (pro-drug for valdecoxib) · Rofecoxib (no longer in use) |
Arachidonic acid pathway:
Prostaglandin receptors:
|
G protein coupled receptor subtypes |
· Gs: ↑cAMP · Gi: ↓cAMP · Gq: ↑IP3 -> ↑ICF [Ca2+], ↑DAG |
|
Prostaglandin receptor subtypes |
· PGD2: Gs, Gi · PGE2: Gq, Gs · PGF2α: Gq · PGI2: Gi · TXA2: Gq, Gs |
The big three:
|
Anti-pyretic |
· ↓PGE2 in hypothalamus |
|
Analgesic |
· ↓PG (especially E2) production at inflamed tissue · ↓Nociceptive receptor activation and expression · ↓Hyperalgaesia and allodynia |
|
Anti-inflammatory |
· ↓PG (especially E2) production by inflamed tissues · ↓Vasodilatation, ↓capillary leak, ↓oedema, ↓WBC chemotaxis · ↓Healing: bone (post fracture), pleura (post pleurodesis) |
Organ systems:
|
Cardiovascular |
·
↓PGI2 -> vasoconstriction,
↑platelet aggregation -> thrombosis e.g. AMI · ↓TXA2 -> vasodilatation, ↓platelet aggregation -> bleeding, bruising · Risk of systemic vasculitis |
|
Respiratory |
· ↓PGD2 -> bronchodilatation · ↓PGE2 -> bronchoconstriction · ↓PGF2α -> bronchodilatation · ↑Shunt of arachidonic acid to leukotrienes -> bronchoconstriction · (overall: bronchoconstriction, ↑in 20% asthmatics) |
|
Gastro-intestinal |
· ↓PGE2 -> ↑parietal cell activity -> ↑HCl secretion · Deranged LFT |
|
Renal |
· ↓PGE2, ↓PGI2 -> ↓tubuloglomerular feedback, ↓renin release o Risk of renal failure, hyperkalaemia o Important if hypovolaemic or also taking ACE inhibitor · ↓Ureteric contraction -> pass kidney stone (indomethacin) · Risk interstitial nephritis |
|
Obstetric |
· ↓PGE2 -> myometrial relaxation · ↓PGF2α -> myometrial relaxation · ↓PGE2 -> closure of ductus arteriosus -> asphyxia |
|
Other |
· Displace other drugs from protein-binding sites, e.g. warfarin on albumin · Metabolic acidosis in overdose |
COX-2 inhibitors:
|
Pros |
· Selective for inflamed tissue (enzyme is inducible cf. constitutive) · ↓Peptic ulceration · ↓Bronchoconstriction · ↓Renal impairment (examiner 2013) · ↓Bleeding risk |
|
Cons |
· ↑Thrombosis risk, AMI (rofecoxib) · ↑Fluid retention · Expensive · Sulfur allergy · Parecoxib is a prodrug with very slow onset of effect |
Feedback welcome at ketaminenightmares@gmail.com