2025ADVANCE Describe the pharmacology of methadone.
tl;dr
· Long-acting multi-modal analgesia confers risks
· Long-acting multi-modal analgesia confers benefits
Physicochemical:
|
Origin |
· First synthesised in Germany… in 1937… |
|
Presentation |
· Oral (tablet, liquid) from any Fitzroy pharmacy · IV methadone HCl 10mg/mL from any proper anaesthetist |
|
Chemistry |
· Synthetic diphenylheptanone · MW 346g/mol · pKa 8.5, 10% unionised · Highly lipid soluble (Octanol:Water 115) |
|
Stereochemistry |
· Racemic mixture · R-methadone: opioid · S-methadone: NMDA antagonist, monoamine reuptake inhibitor, ↑QTc |
Pharmacokinetic
|
Administration |
· PO · IV, IM, SC |
|
Time course |
· Onset: within minutes ·
Peak: analgesia 10 mins, resp depression ?30mins · Duration: dose-dependent o 10mg: few hours o 20mg: 1 day o 30mg: 3 days |
|
Absorption |
· Oral bioavailability 75%: low first pass hepatic metabolism · Variable time to peak effect 1-5 hours |
|
Distribution |
· Highly bound to plasma proteins (α1AG, 90%) · Extensively distributed (VDss 6L/kg) · Moderately quick distribution to tissues (t1/2α 6 mins) · Moderately quick equilibration with CNS (t1/2ke0 8 mins) · Crosses placenta. Pregnancy Class C · Small amounts in breast milk (N.B. minimal intake in first week FML) |
|
Metabolism |
Pathways: · Hepatic Phase 1 N-demethylation · 2B6, 3A4 > 2C19, 2C9, 2D6 · Major metabolite inactive (EDDP -> EMDP) · Minor metabolite weakly active (nor-methadol) Speed: · Longest duration of all opioids · Cl 6mL/kg/min · t1/2β 15-60 hours, mean 1 day Variability: · Significant 2B6 polymorphism (also 2C19, 2D6 but less important) · Reduced function alleles common worldwide · Oceania (60%) > Africa (40%) > Europe (30%) > Asia (20%) · Affects S-methadone >> R-methadone · Repeat dosing -> ↑↑[S-methadone] -> ↑QTc, ↑5HT · Minimal effect on duration of opioid activity |
|
Excretion |
· Parent -> Urine (10%) o ↑ if ↓pH (up to 30%) · Metabolites -> bile, urine |
Pharmacodynamic
|
Receptor effects |
· Full μ opioid agonist · NMDA antagonist (contribution unknown, likely less than ketamine) · NAd and 5HT reuptake inhibitor · hERG* Cardiac K+ channel inhibitor
*hERG = human ether-a-go-go related gene |
|
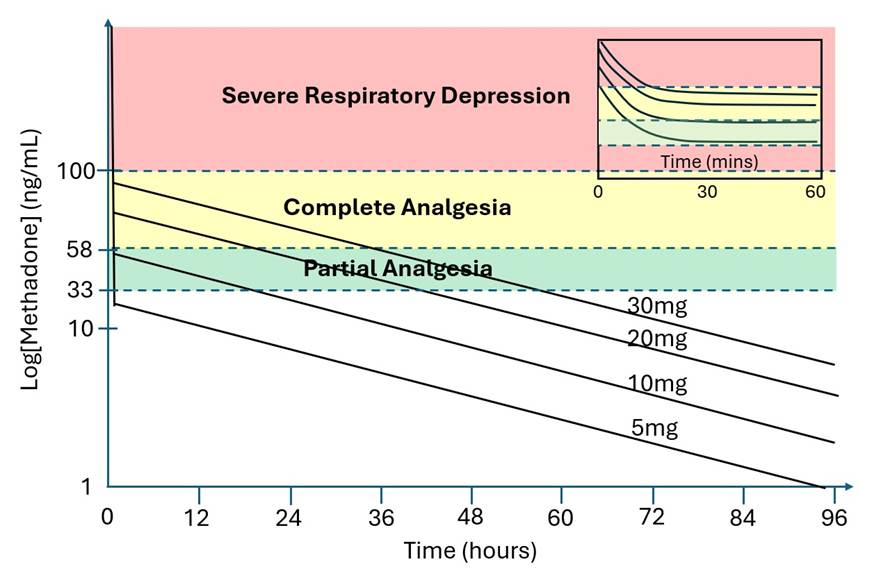
Thresholds |
· Severe Resp Depression: ~100ng/mL · Complete Analgesia: ~60ng/mL · Partial Analgesia: ~30ng/mL |
|
Uses |
· Acute & chronic pain · Somatic & visceral & neuropathic pain · Evidence base across many surgical specialties · Opioid addiction & withdrawal |
|
Benefits |
· ↓Opioid side effects (cf. pure opioids at equi-analgesic doses) · ↓Opioid use (up to 3/12 post-op) · ↓Pain scores (up to 3/12 post-op) · The above could reduce the risk of long-term use and addiction |
|
Respiratory depression |
· Especially with benzodiazapines, gabapentinoids · Especially if sleep-disordered breathing · Partial reversal of effect with naloxone · Highest risk 30-45 mins (cf. intrathecal morphine 6-12 hours) |
|
Serotonin syndrome |
· It’s real and I’ve seen a mild variant from a single dose · Mostly with high doses and repeat doses · Mostly if combined with other serotonergic drugs · Mostly if multiple mechanisms · Worst: MAOi (14 days offset), tramadol, pethidine (MAOis: methylene blue, moclobemide, selegiline) |
|
Torsades de Pointes |
· Inhibits cardiac K+ channels -> ↑QTc and ↑risk TdP · Risk factors: Congenital long QT, Class 3 antiarrhythmic, ↓K+, ↓Mg2+ · Mostly (but not always) with repeated high dose (>100mg/day) · Could be mimicked with a big IV push |
PK & PD:
User’s Guide:
|
Dosing |
· Day case: 5-10mg (e.g. elective lap chole. Is it worth it?) · Overnight stay: 10-20mg (e.g. joint replacement) · ICU major: 20-30mg (e.g. liver resection) |
|
Timing |
· Give a bit at a time, e.g. 2-3mg q2-3 mins · Give most of it early: anaesthetic room vs induction vs pre-incision · Give a small top up at end of case if needed · Titrate against pupil size, RR, PaCO2 at steady state |
|
Adjuvants |
Pure Opioids: Careful · Induction: use short-acting opioid · Recovery: as usual · Ward: as usual. Lower dose or PCA if concerned. · Long acting: no intrathecal morphine. No slow-release opioid. Benzodiazepines: Careful · Kharasch advises extreme caution · Avoid if short procedure / day case / sleep-disordered breathing · Small dose (0.5-2mg) ok when lining up for a long & major procedure · Opioids aren’t anxiolytic, come at me Alph 2 Agonists: Careful · Kharasch advises extreme caution · Clonidine: too sedating, too long-acting · Dexmed: must use EEG to titrate anaesthetic agent Ketamine: Yes · Significant additional analgesic benefit · Minimal respiratory depression · Give as you normally would |
|
Anaesthetic |
Wakeup Strategies: (for long procedure + comfortable patient) · Processed EEG for titration · Sevoflurane -> propofol +/- remifentanil (mid-procedure switch) · Sevoflurane -> desflurane (mid-procedure switch, if you’re evil) · (Sevoflurane’s 90% decrement time climbs steeply after 2 hours) |
Credits
Thanks to Harsh Dubey for teaching me the most out of anyone
Thanks to John Webster for his excellent literature review
Thanks to Evan Kharasch for resurrecting and advancing this topic
Thanks to Geoffrey Gourlay for his pioneering work
Thanks to Sarah Lee for organising this whole thing
Feedback welcome at ketaminenightmares@gmail.com