2021A06 Compare and contrast the pharmacology of metaraminol and adrenaline (epinephrine).
Physicochemical:
|
|
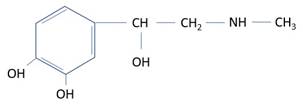
Adrenaline |
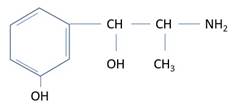
Metaraminol |
|
Structure |
|
|
|
Structure-activity |
· Catecholamine: direct, potent, sensitive to COMT · OH on β-carbon: direct, alpha · No substitution on α-carbon: MAO sensitive · Larger amine: β>α |
· Non-catecholamine: resistant to COMT · OH on β-carbon: direct, alpha · CH3 substitution on α-carbon: indirect, MAO resistant · Smaller amine: α>β |
|
Presentation |
· 1mg in 1mL or 10mL (concentrated ++++) |
· 10mg in 1mL (concentrated++) |
|
Tissue necrosis |
· High risk – CVC only |
· Low risk – PIVC ok |
Pharmacokinetic:
|
|
Adrenaline |
Metaraminol |
|
Administration |
· IV infusion: 1-30mcg/min · IV bolus: 1mg in cardiac arrest · IM bolus: 500mcg in anaphylaxis |
· IV bolus: 0.5-1mg (10-20mcg/kg) PRN · IV infusion: typically 0.5-5mg/h (20-200mcg/kg/h) · S/C or IM |
|
Time course |
· Onset < 1min · Duration 5 mins o Drug elimination rapid o Receptor effects prolonged |
· Onset 1-2 min · Duration: stated 20-60mins, likely shorter |
|
Absorption |
· Not orally bioavailable |
· Orally bioavailable, % unknown |
|
Distribution |
· VD 0.1-0.2L/kg · 12% protein bound · Should not cross blood-brain barrier |
· Poorly studied in humans · 45% protein bound · VD 4L/kg · Should not cross BBB |
|
Metabolism |
· By COMT and MAO -> VMA · By COMT only -> normetadrenaline · t1/2β 2 mins |
· Poorly studied in humans; likely slow · Not susceptible to MAO or COMT · t1/2β 6 hours |
|
Excretion |
· Metabolites -> urine |
· Unknown |
Pharmacodynamics:
|
|
Adrenaline |
Metaraminol |
|
Receptor activity |
· β1 > β2 > α1 · Direct only (i.e. via adrenoceptors) |
· α1 >> β1 · Direct and indirect o Displaces noradrenaline from vesicles |
|
Use |
· Anaphylaxis (↑CO, ↑SVR, stabilize mast cells) · Cardiogenic shock (↑CO) · Cardiac arrest (↑SVR -> vital organ perfusion) · Additive with local anaesthetic (↑duration, ↓LAST) |
· Peri-operative hypotension – GA and neuraxial · Unclear if equivalent to phenylephrine in obstetrics |
|
Toxicity |
· Safer with noradrenaline reuptake inhibitors (NRI) · Tachyphylaxis slow: adrenoceptor downregulation |
· Dangerous with NRI e.g. MAOi (↑↑NAd release) · Tachyphylaxis rapid: catecholamine depletion |
Feedback welcome at ketaminenightmares@gmail.com