2020A06Describe how the effects of warfarin can be reversed
when URGENT surgery is indicated (40%).
For each option discuss the advantages and disadvantages
(60%).
Intro:
|
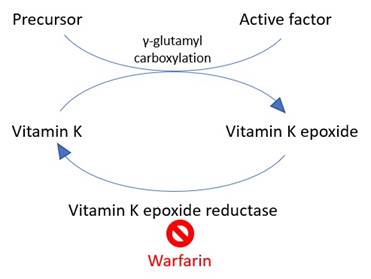
Mechanism |
· Vitamin K epoxide reductase inhibitor
|
|
Factors affected (half life) |
· Procoagulants: II (60h), VII (6h), IX (24h), X (36h) · Anticoagulants: protein C (8h), protein S (30h) |
Reversal considerations:
|
Determinants |
· Urgency of surgery · Active bleeding · Degree of reversal required (e.g. neuraxial vs superficial) |
|
Monitoring |
· INR is sensitive to factor VII (short t1/2) >> factor II (long t1/2) · Hence INR will normalise before coagulation is restored
·
Hence need INR ≤1.2 for safe neuraxial block
after stopping warfarin |
Reversal options:
|
1.Expectant |
· i.e. drug washout -> regenerate Vit K -> regenerate clotting factors · t1/2β 40 hours -> offset in 5 days · ↑Duration if: Vit K deficient e.g. malnourished, CYP inhibitor (e.g. cimetidine), CYP competition e.g. amiodarone · ↓Duration if: CYP inducer (e.g. barbiturates) · Can operate immediately if a) low risk of bleeding b) benign consequences of bleeding c) easily compressible site · Pro: ↓risk thrombotic events, less disruptive to patient · Con: slow offset, ↑risk surgical bleeding |
|
2.Vitamin K |
· i.e. replenish substrate -> regenerate clotting factors · PO 1-2mg for effect in 12-24 hours · IV 5-10mg for effect in 6-12 hours · Pro: fairly rapid reversal, obviates risks of blood products · Con: insufficient if very high INR or if active bleeding, difficult to restart warfarin after a big dose of Vitamin K |
|
2.FFP |
· Contains all clotting factors · IV 15-30mL/kg (or 2-4mL/kg if with prothrombinex) · Also give Vit K to avoid rebound anticoagulation · Pro: immediate · Con: 15-30mL/kg = risk of TACO, risks of allogeneic transfusion |
|
3.Prothrombinex |
· Contains factors 2, 9, 10 · IV 25-50 units/kg · Also give Vit K to avoid re-bound anticoagulation · Pro: immediate, universally compatible · Con: factor 7 absent in Australian PCC |
|
4.FEIBA |
· Contains active factor 7a, inactive factors 2,9,10 · IV 50-100 units/kg · Also give Vit K to avoid rebound anticoagulation · Pro: contains all deficient coag factors · Con: less data for warfarin reversal |
|
5.Novoseven |
· Activated Factor 7a · IV 50mcg/kg · Given in addition to FFP and/or prothrombinex · Only if persistent uncontrollable haemorrhage despite all other physiological, pharmacological and surgical efforts · Pro: immediate · Con: very expensive, short half life, high risk of thrombotic complications |
Feedback welcome at ketaminenightmares@gmail.com