2001A12 Briefly describe the respiratory effects of the volatile agents.
List:
· A: airway reflexes
· B: respiratory depression
· C: pulmonary circulation
· D: excitation
A: airway:
|
Physicochemical |
· Isoflurane, desflurane: irritation -> laryngospasm, coughing, secretions · Sevoflurane, halothane, enflurane -> gas induction well tolerated |
|
Bronchodilatation |
· ↓L-Ca2+, ↑NO activity · ↓Airway resistance, ↓work of breathing; use in status asthmaticus · ↑Anatomical dead space (not clinically significant) |
|
↓Airway reflexes |
· Tolerate LMA · ↑Risk aspiration |
|
↓Pharyngeal dilator tone |
· Skeletal muscle relaxation -> airway obstruction (especially if OSA) |
|
↓Ciliary activity |
· ?↑Risk pneumonia |
B: respiratory depression
|
Summary |
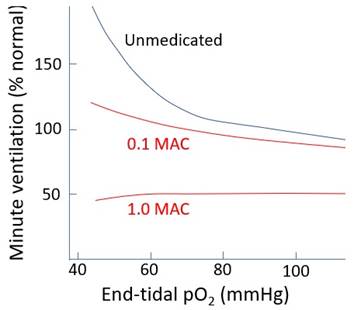
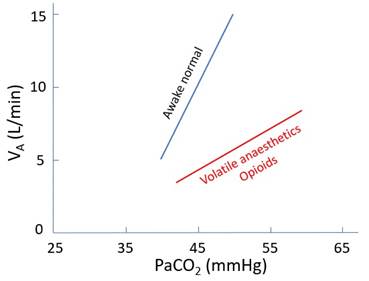
· ↑RR, ↓VT · ↓MV, ↑PaCO2 (~50mmHg at 1 MAC) · ↓Response to ↑PaCO2 · ↓↓Response to ↓PaO2
·
Respiratory arrest at high concentration · Enflurane > isoflurane/desflurane > sevoflurane > halothane |
|
Response curves |
|
|
Mechanisms |
· Respiratory centre depression o ↑GABA, ↑glycine in brainstem · Chemoreceptor depression o ? mechanism · Skeletal muscle relaxation o Affects intercostals > diaphragm o ↑Glycine, ↑GABA: ↓spinal cord α-motor neuron output o Inhibition of L-Ca2+ channel: ↓force of contraction o Inhibition of post-synaptic nAChR at NMJ o Inhibition of pre-synaptic VDCC at NMJ |
C: pulmonary circulation
|
↓HPV |
· Inhibition of L-Ca2+ channel, ↑NO release · Pulmonary vasodilatation · ↓PVR, ↓HPV · ↑V/Q mismatch -> ↓PaO2 |
|
↑Dead space |
· ↓Venous return -> ↓RV output · ↓PASP -> ↑West zone 1 i.e. alveolar dead space · ↑PaCO2 – etCO2 difference |
|
Carbon monoxide poisoning |
· Desflurane > isoflurane = enflurane · Reaction with CO2 absorber · HbCO can rise to 35% · Risk factors: ↓FGF, ↑temp, exhausted absorber, baralyme > sodalime |
D: excitation
i.e. Guedel’s stage 2: at concentration just above MAC-awake
|
Airway |
· ↑Sensitivity to stimulation · Coughing, laryngospasm, bronchospasm, regurgitation/aspiration |
|
Breathing |
· ↑↑RR · Irregular breathing, breath holding |
Feedback welcome at ketaminenightmares@gmail.com