2004A01 Describe
the effects of isoflurane on intracranial metabolism, intracranial
haemodynamics, intracranial pressure and the EEG.
List:
· Graphs: CMRO2, CBF, anaesthesia
· EEG effects
· CSF circulation effects
Metabolism and haemodynamics:
|
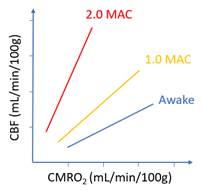
CBF vs CMRO2 |
· Dose-dependent vasodilatation (↓L-Ca2+ activity, ↑NO activity) · Coupling of CBF and CMRO2 impaired (not ablated)
· Slope ∝ dose -> greater effect at high dose
|
|
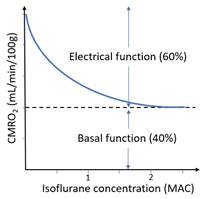
CMRO2 vs MAC |
· Dose-dependent reduction in electrophysiological function (60% of total) · No effect on basal function (40% of total) – only reduced by hypothermia
· Exponential decay -> greater effect at low dose
|
|
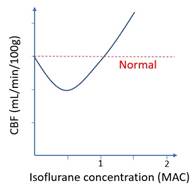
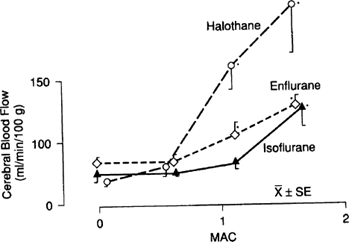
CBF vs MAC*** |
· At low concentration: indirect vasoconstriction (via ↓CMRO2) wins · At high concentration: direct vasodilatation wins
|
|
Other |
· Luxury perfusion: due to ↓CMRO2 but ↑CBF · Hypoventilation: ↑PaCO2 may cause further vasodilatation (if spont vent) |
EEG effects:
|
Changes |
· ↑Amplitude o Due to relative synchronization -> summation · ↓Frequency: o β (12-30Hz) -> α (8-12Hz)-> θ (4-8Hz)-> δ (0-4Hz) o Burst suppression at ~1.5MAC o Electrical silence at ~2 MAC o Ablation of seizures o ↓BIS and entropy scores · Guedel’s stage 2: opposite changes o ↑Frequency, ↓Amplitude |
|
Causes |
· ↓Activity of ascending reticular activating system (ARAS) · Disinhibition of thalamic pacemaker cells -> rhythmic discharge · Shift from complex and quasi chaotic to simple and predictable activity · Summation of identical waveforms results in increased amplitude |
CSF effect:
|
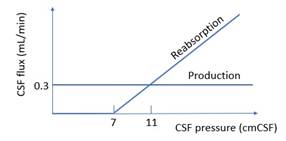
↓Production |
· If mAP <70mmHg |
|
↑Reabsorption |
· If ↑CBF -> ↑ICP |
|
|
Note: X axis unit mmCSF not mmHg Note: Y axis zero point not at the X axis |
Addendum***
· This graph is from Miller’s Anesthesia, Chapter 11
· The data are from Anesthesiology (https://pubmed.ncbi.nlm.nih.gov/3740503/)
· At 0.5 MAC, mean values for local blood flow were reduced in every grey matter tissue
· However, none of the individual changes was statistically significant due to a large standard deviation
· My personal opinion is:
o It is unlikely that a universal decrement in mean blood flow between 0 MAC and 0.5 MAC was due to chance
o Statistical significance would have been reached had sample sizes been larger
o These findings are consistent with the curves for CBF vs CMRO2 and CMRO2 vs MAC
· The alternative opinion is:
o There is no evidence for significant change in CBF between 0 MAC and 1 MAC
o In this range, the indirect vasoconstriction (via ↓CMRO2) and the direct vasodilation roughly cancel each other out
o This is consistent with the leftward/upward shift in the CBF vs mAP curve that occurs with any concentration of volatile anaesthetic
o See the Eger-Stoelting version below:
Special thanks to Dr. Stan Tay for his insights.