2019A10 Describe
the effects of sevoflurane on the following regional circulations:
cerebral, coronary, pulmonary, hepatic and uteroplacental. Do not discuss
specific organ effects.
Intro:
· Flow physiology
· Cellular
· Systemic
· Regional
Flow physiology:
|
Ohm’s law |
· Flow rate = (P1 – P2) / resistance |
|
Poiseuille’s law |
· Resistance to laminar flow = (8 x length x viscosity) / (π x radius4) · Hence radius is the major factor |
Cellular effects:
|
Central |
↑GABA/glycine activity -> ↓SNS output from medulla · ↓Inotropy · ↓Vasoconstriction · ↓Venoconstriction · Note relative preservation of baroreceptor reflex |
|
Peripheral |
· ↓L-Ca2+ activity, ↓SR Ca2+ release · ↑KATP activity · ↑NO release -> · ↓Vasoconstriction · ↓Venoconstriction |
Systemic vascular effects: (dose-dependent)
|
Direct |
· ↓Inotropy -> ↓cardiac output · ↓Vasoconstriction -> ↓SVR, ↓PVR · ↓Venoconstriction -> ↓MSFP -> ↓preload -> ↓cardiac output |
|
Indirect |
· Baroreceptor reflex o ↑Heart rate -> ↑cardiac output nearer to normal · Excitation (Guedel’s stage 2) o ↑SNS output -> ↑HR, ↑mAP |
Cerebral circulation:
|
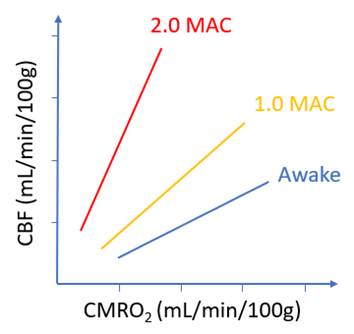
CBF vs CMRO2 |
· Dose-dependent vasodilatation · Coupling of CBF and CMRO2 impaired (not ablated)
· Slope ∝ dose -> greater effect at high dose
|
|
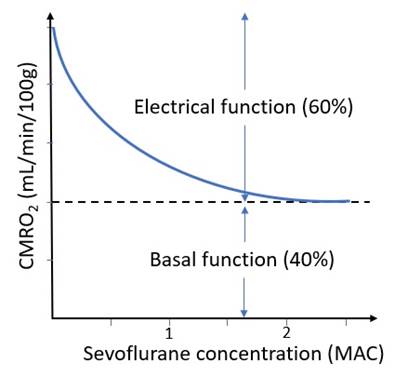
CMRO2 vs MAC |
· Dose-dependent reduction in electrophysiological function (60% of total) o Burst suppression at ~1.5 MAC o Isoelectricity at ~2 MAC · No effect on basal function (40% of total) – only reduced by hypothermia
· Exponential decay -> greater effect at low dose
|
|
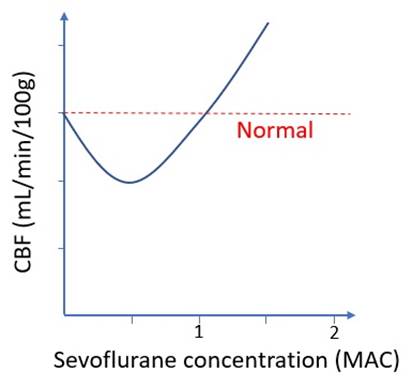
CBF vs MAC*** |
· At low concentration: indirect vasoconstriction (via ↓CMRO2) wins · At high concentration: direct vasodilation wins · Important if already raised ICP (e.g. intracranial bleed)
|
|
Other |
· Luxury perfusion: due to ↓CMRO2 but ↑CBF · Hypoventilation: ↑PaCO2 may cause further vasodilatation (if spont vent) |
Coronary circulation:
|
Factors increasing flow *predominant* |
· Metabolic autoregulation: ↑HR -> ↑MVO2 · Direct vasodilatory effect · ↓SNS output |
|
Factors decreasing flow *outweighed* |
· Metabolic autoregulation: ↓SVR/wall tension, ↓contractility -> ↓MVO2 · ↓Aortic root DBP -> ↓perfusion pressure |
|
Coronary steal syndrome |
· Stenotic vessels are maximally dilated when awake · Other vessels dilate under volatile GA · Blood is ‘stolen’ from already threatened myocardium · Only relevant if steal-prone anatomy · More likely with isoflurane · Not clinically significant |
|
Anaesthetic preconditioning |
· Mimic of ischaemic preconditioning · Due to activation of K+ATP channel (vascular/mitochondrial/sarcolemma) · Onset in minutes, offset 3-4 days |
Pulmonary circulation:
|
Effects |
· Direct vasodilatation · ↓SNS output -> vasodilatation · ↓PVR · ↓Pulmonary artery pressure |
|
Significance |
· Impaired HPV -> ↑V/Q mismatch · ↓PASP -> ↑alveolar dead space, ↑West zone 1 |
Hepatic circulation:
|
Factors increasing flow |
· Direct vasodilatation · ↓SNS output -> vasodilatation |
|
Factors decreasing flow |
· ↓mAP -> ↓perfusion pressure |
|
Significance |
· Unimportant at usual partial pressure · Preserved hepatic arterial buffer response (?) |
Uteroplacental circulation:
|
Factors increasing flow |
· Direct vasodilatation · ↓SNS output -> vasodilatation (but vessels are already maximally dilated) |
|
Factors decreasing flow |
· ↓mAP -> ↓perfusion pressure |
|
Significance |
· Pressure-passive circulation · Risk of foetal asphyxia under GA |
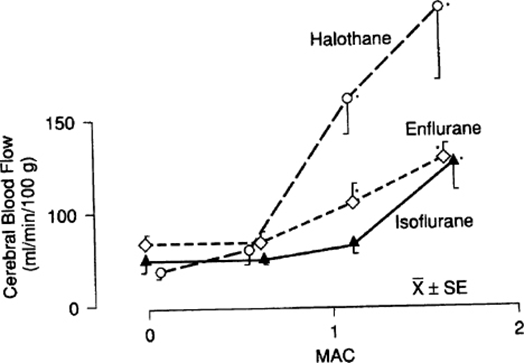
Addendum***
· This graph is from Miller’s Anesthesia, Chapter 11
· The data are from Anesthesiology (https://pubmed.ncbi.nlm.nih.gov/3740503/)
· At 0.5 MAC, mean values for local blood flow were reduced in every grey matter tissue
· However, none of the individual changes was statistically significant due to a large standard deviation
· My personal opinion is:
o It is unlikely that a universal decrement in mean blood flow between 0 MAC and 0.5 MAC was due to chance
o Statistical significance would have been reached had sample sizes been larger
o These findings are consistent with the curves for CBF vs CMRO2 and CMRO2 vs MAC
· The alternative opinion is:
o There is no evidence for significant change in CBF between 0 MAC and 1 MAC
o In this range, the indirect vasoconstriction (via ↓CMRO2) and the direct vasodilation roughly cancel each other out
o This is consistent with the leftward/upward shift in the CBF vs mAP curve that occurs with any concentration of volatile anaesthetic
o See the Eger-Stoelting version below:
Special thanks to Dr. Stan Tay for his insights.