2006B03 Describe
the factors which contribute to the inter-individual variability in drug
response seen with intravenous induction agents.
List:
· Intro
· Kinetics/biophasics
· Dynamics
Intro:
|
IV induction drugs |
· Propofol: 1-2mg/kg · Thiopentone: 3-7mg/kg · Ketamine: 1-2mg/kg · Etomidate: 0.3mg/kg · Midazolam: 0.3mg/kg |
|
Problems |
· The three compartment model poorly describes induction kinetics · Variable relationship between dose and concentration (= kinetics) · Variable relationship between concentration and effect (= dynamics) |
|
Implications |
· Risk of overdose -> hypotension · Risk of underdose -> risk of awareness · Propofol TCI models are inaccurate at induction |
Pharmacokinetics / pharmacobiophasics:
|
Time course |
· Kinetics = administration -> plasma concentration (Cp) o Three compartment model inaccurate o Mostly patient-dependent delay · Biophasics = plasma concentration -> effect site concentration (Ce) o Modelled by t1/2ke0 o Mostly drug-dependent delay |
|
Onset |
Speed of LOC ∝ (magnitude of peak effect) / (time to peak effect)
(A) Magnitude of peak effect ∝ · ↑Dose size · ↑Speed of injection (bolus cf. TCI injection) · ↓Cardiac output (↑pregnant/neonate/obese, ↓elderly/shock) · ↓Central blood volume (↑pregnant/obese/neonate, ↓elderly/shock) · ↑Speed and extent of recirculatory second peak (important if bolus is slow)
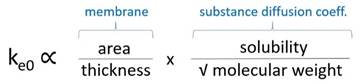
(B) Time to peak effect ∝ · ↑Rate of delivery to effect site o ↑Cardiac output (note bivalent effects) o ↓Distance from injection site to brain (e.g. CVC cf. lower limb PIVC) · ↑Rate of effect site equilibration (↑ke0 -> ↓t1/2ke0)
o ↓Thickness (e.g. immature BBB in neonate) o ↑Lipid solubility (e.g. thiopentone – t1/2ke0 1 min – hence clear endpoint) o ↑% Unionized (e.g. propofol >99% - t1/2ke0 2.6 mins) |
|
Offset |
Speed of offset ∝ distribution x metabolism x excretion
(A) Distribution ∝ · ↑Cardiac output / compartment blood flow (as above) · ↑Compartment volume (↑obesity/bodybuilders, ↓cachexia) · ↑Compartment-to-blood partition coefficient
(B) Metabolism: rarely important after induction bolus · e.g. thiopentone: zero order kinetics -> hang-over effect
(C) Excretion rate: unimportant after induction bolus · e.g. ketamine: accumulation of norketamine metabolite in renal failure |
Dynamics:
|
Time course |
· Dynamics = effect site concentration -> effect o Represented by dose response curve o Effect on brainstem, thalamus, cerebral cortex o Minimal delay |
|
Physiology |
· Neonate: immature brain structures -> ↓Cp50 · Elderly: ?↓ion channel function, ?↓ synaptic activity -> ↓Cp50 · Pregnancy: progesterone -> ↓Cp50 · Obesity: inflammatory cytokines -> ↓Cp50 · Anxiety -> ↑SNS -> ↑Cp50 |
|
Pathology |
↓Cp50 if: · ↓mAP (<40mmHg) · ↓pO2 (<40mmHg) · ↑pCO2 (>60mmHg sedation, >80mmHg anaesthesia if acute) · ↓Temp · ↓pH ↑Cp50 if: · ↑Temp |
|
Drug interaction |
· Synergistic: e.g. fentanyl 1mcg/kg reduces dose of propofol by 20% · Additive: e.g. ↓propofol Cp50 co-induction with volatile agent · Infra-additive: e.g. ketamine + midazolam · Antagonistic: e.g. propofol + acute amphetamine · Tolerance: e.g. chronic barbiturate use |
|
Pharmacogenomic |
· e.g. propofol Cp50 for immobility is 15mcg/mL with std dev 5mcg/mL · Polymorphism of receptor structure and number, ion channels, ICF signalling |
|
Idiosyncratic |
· Propofol: myoclonus in 10% · Thiopentone: acute intermittent porphyria rarely · Etomidate: severe PONV common · Ketamine: post-op delirium in 30% |
Feedback welcome at ketaminenightmares@gmail.com