2014A02 Draw and
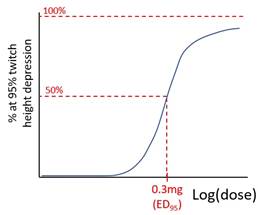
explain the characteristics of a log dose response curve
that describes the major clinical effect of rocuronium.
Describe how factors encountered in clinical practice may alter this curve.
List:
· Graph
· Intro
· Factors ↑ED95 = R shift = ↓potency
· Factors ↓ED95 = L shift = ↑potency
· Factors ↑duration (not relevant here)
Graph:
Population, quantal curve
Intro:
|
Rocuronium |
· Non-depolarising relaxant · Competitive inhibitor at α-subunit of nAChR at NMJ · Must bind 70% of receptors before significant effect due to spare receptors |
|
Measured responses |
· Onset time (time to 95% ↓single twitch height) · Depth (minimum post-tetanic count?) · Offset time (time to TOF ratio 0.9) |
|
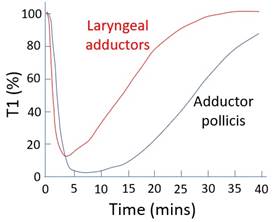
Muscle group differences |
Laryngeal muscle cf. adductor pollicis: · Physiological differences: o ↑Blood flow o ↑ACh vesicle release o ↑ACh receptors · Clinical implication: o Faster onset o Less depth o Shorter duration
|
|
Implications of inter-individual differences |
· ↑Potency and ↑duration: failure of reversal -> distress, T2RF, aspiration · ↓Duration: movement when dangerous e.g. neurosurgery · Twitch monitoring essential whenever relaxants used |
Factors ↑ED95 = R shift = ↓potency:
|
Physiology |
· ↑K+: membrane depolarisation-> ↑ACh release -> ↓drug:ACh ratio |
|
Pathology |
· Critical illness myopathy, burns -> proliferation of extrajunctional receptors -> ↓drug:ACh ratio · Malignant hyperthermia-> post-junctional activation |
|
Competitive reversal |
· AChEi e.g. neostigmine: ↓drug:ACh ratio (g-cyclodextrin chelates rocuronium in plasma, increases the gradient between effect site and plasma but does not alter the dose-response curve) |
|
Toxins |
· Tetanus toxin: ↓inhibition of a-motor neurons -> ↑NMJ activity -> ↓drug:ACh ratio |
Factors ↓ED95 = L shift = ↑potency
|
Physiology |
↓ACh release -> ↑drug:ACh ratio · Neonate: immature NMJ · Respiratory acidosis · ↑Mg2+: ↑competition with Ca2+ · ↓K+: membrane potential more negative -↓ACh release |
|
Pathology |
· Myasthaenia gravis: antibody against NMJ nAChR -> ↑drug:receptor ratio · Lambert-Eaton syndrome: antibody against pre-synaptic VDCC -> ↓competition with ACh |
|
Pre-synaptic drugs |
↓ACh release -> ↑drug: ACh ratio · ↓α-motor neuron activity: volatile anaesthetic · ↓ axonal action potential: peripheral nerve local anaesthetic (↓Na+ flux) · ↓Choline uptake: hemicholinium · ↓ACh transport into vesicles: vesamicol · ↓AMP/ATP synthesis (frusemide) · Block pre-synaptic nAChR (volatiles) · Block L-Ca2+ (CCB, Mg2+, aminoglycosides, volatiles) |
|
Post-synaptic drugs |
↓Ion flux through nAChR · Block post-synaptic nAChR: other non-depolarisers, volatiles, aminoglycoside, quinidine · Desensitisation blockade (volatiles, barbiturates) · Inhibit peri-junctional action potential: local anaesthetic ↓Na+ flux |
|
Post-junctional drugs |
· Dantrolene: inhibit skeletal muscle ryanodine receptor |
|
Toxins |
· Botox: cleave SNARE protein, ↓ACh release · Tetrodotoxin: VDNaC inhibition |
Addit: factors increasing duration
*All those causing ↑potency plus…*
|
Pathology |
· ↓Temp: ↓rate of Hoffman degradation and ester hydrolysis · ↑pH: ↓rate of ester hydrolysis · ↓pH: ↓rate of Hofmann degradation · Atracurium: 60% ester hydrolysis, 30%, Hoffman elimination, 10% in urine unchanged · Cisatracurium: 80% Hoffman elimination, 15% ester hydrolysis, 5% in urine unchanged |
|
Pathology |
· Liver failure: accumulation of bile eliminated drug (e.g. vecuronium 70%) · Renal failure: accumulation of drug (e.g. gallamine 100% renal), metabolite (e.g. 3-OH-panc 50% potency) |