2019A12 Outline the factors that determine the rate of recovery from non-depolarising neuromuscular block.
List:
· Intro
· Dose = starting [drug]
· Biophasics = rate of transfer from effect site to central compartment
· Kinetics = rate of ↓[drug]
· Dynamics = [drug] for offset (could technically write about ↑sensitivity and ↓sensitivity)
Intro:
|
Determinants of time to recovery |
· Final effect site concentration after bolus or at end of infusion · Rate of removal from effect site · Rate of elimination from the plasma · Effect site concentration required for recovery of neuromuscular function |
|
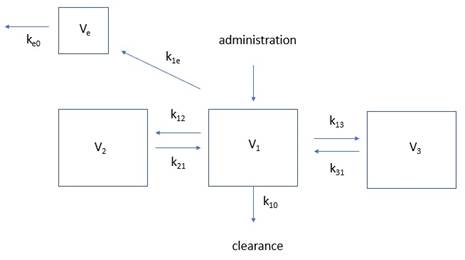
Compartment model |
|
|
Standard |
· Train-of-four ratio 0.9 (or return to 25% baseline twitch height?) |
|
Usual duration |
· 30-45 mins for 2x ED95 · 45-60 mins for 4x ED95 |
Ce after bolus or at end of infusion (factors increasing it)
|
Administration |
· ↑Bolus size (e.g. 4x ED95 rocuronium cf. 2x ED95) · ↑Infusion rate · ↑Infusion duration |
|
Drug |
· ↓Elimination rate (see below) |
|
Patient |
· ↓Volume of distribution (see below) |
Removal from effect site:
|
Fick’s law |
|
|
Chelation reversal |
· γ-cyclodextrin chelates rocuronium > vecuronium >> pancuronium o Interaction occurs in plasma, not receptor site o ↓C2 -> ↑concentration gradient -> ↑rate of removal o i.e. kinetic not dynamic interference · Dosing o 16mg/kg immediately after intubating dose o 4mg/kg moderate blockade o 2mg/kg minimal residual blockade |

Elimination from central compartment: (factors slowing it)
|
Short infusion |
Offset during distribution phase · ↓Cardiac output (e.g. shock) · ↓Volume of distribution o ↓Muscle mass (e.g. elderly, cachectic) o ↑Water mass (e.g. hypovolaemia) |
|
Long infusion |
Offset during terminal elimination phase · ↑Cardiac output (e.g. pregnant, neonate) · ↑Volume of distribution o ↑Muscle mass (e.g. athletic) o ↑Water mass (e.g. heart failure, renal failure, liver failure) · ↓Metabolism o ↓Phase 1,2 reactions (e.g. liver failure) -> ↑duration aminosteroids o ↓Hoffman degradation (↓temp, ↓pH) -> ↑duration benzylisoquinoliniums o ↓Ester hydrolysis (↓temp, ↑pH) -> ↑duration benzylisoquinoliniums · ↓Excretion of drug or active metabolite o ↓Renal excretion (renal failure -> accumulate pancuronium, gallamine) o ↓Biliary excretion (liver failure -> accumulate vecuronium, rocuronium) |
*Note: muscle relaxants have a very small VDSS; my understanding was that
distribution is unimportant,
but the examiner’s report suggests otherwise*
Ce at which offset occurs: (factors decreasing it)
|
Muscle group |
· Laryngeal adductors recover before adductor pollicis due to o ↑Blood flow o ↑ACh vesicles released o ↑Number of receptors |
|
Physiological factors |
↓ACh release -> ↑drug:ACh ratio · Neonate: immature NMJ · Elderly: ↓ACh spare receptors · ↑Mg2+: antagonize Ca2+ at pre-synaptic L-Ca2+ channel · ↓K+: hyperpolarization · Hypothermia · Resp acidosis |
|
Pathological factors |
· Myasthaenia gravis (↓↓spare receptors) · Lambert-Eaton syndrome (antibody against VDCC, ↓ACh released) (note: denervation -> upregulation of extra-junctional receptors -> ↑Ce for offset) |
|
Pre-synaptic drugs |
· ↓α-motor neuron activity: volatile anaesthetic · ↓ axonal action potential: peripheral nerve local anaesthetic (↓Na+ flux) · ↓Choline uptake: hemicholinium · ↓ACh transport into vesicles: vesamicol · ↓AMP/ATP synthesis (frusemide) · Block pre-synaptic nAChR (volatiles) · Block L-Ca2+ (CCB, Mg2+, aminoglycosides, volatiles) |
|
Post-synaptic drugs |
· Block post-synaptic nAChR: other non-depolarisers, volatiles, aminoglycoside, quinidine · Desensitisation blockade (volatiles, barbiturates) · Inhibit peri-junctional action potential: local anaesthetic ↓Na+ flux |
|
Post-junctional drugs |
· Dantrolene: inhibit skeletal muscle ryanodine receptor |
|
Toxins |
· Botox: cleave SNARE protein, ↓ACh release · Tetrodotoxin: VDNaC inhibition |
Ce at which offset occurs: factors increasing it
|
Physiology |
· ↑K+: membrane potential less negative -> ↑ACh release -> ↓drug:ACh ratio |
|
Pathology |
· Critical illness myopathy, burns -> proliferation of extrajunctional receptors -> ↓drug:ACh ratio · Malignant hyperthermia-> post-junctional activation |
|
Competitive reversal |
· Acetylcholinesterase inhibitor (e.g. neostigmine -> ↑ACh:Drug ratio -> displacement · Obtain train-of-four ratio of >0.9 earlier · Should not be given until three TOF twitches |
|
Toxins |
· Tetanus toxin: ↓inhibition of a-motor neurons -> ↑NMJ activity -> ↓drug:ACh ratio |
Feedback welcome at ketaminenightmares@gmail.com