2019B06 Propofol and
remifentanil TCI are often given together as a TIVA technique.
Discuss pharmacological reasons why this is a useful
combination.
List:
· Summary
· Drug effects
· PD
· PK
· PC
· Applications
Summary:
|
Pharmacodynamic (PD) |
· Complementary and synergistic -> ↓dose -> ↓side effects |
|
Pharmacokinetic (PK) |
· Ideal properties of each · No interference · Synergistic -> ↓dose -> ↓accumulation |
|
Pharmaceutic (PC) |
· Compatible |
Drug effects:
Pharmacodynamics:
|
Complementary |
· PPF: anaesthesia · RF: analgesia |
|
Synergistic |
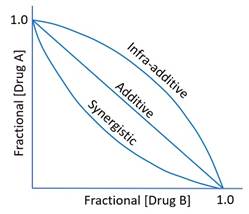
· Combined effect exceeds sum of individual effects · Represented by isobologram (or response surface) · Mechanism: ? RF reduces nociceptive activation of ascending reticular activating system (ARAS)
|
|
Implications of synergism |
· ↓PPF Cp50 for hypnosis and immobility · ↓Ceγ -> ↓PPF Cp50 variability (?) · ↓PPF side effects · ↓Need for paralysis |
Pharmacokinetics:
|
PPF ideal features |
· Rapid onset: o Small o High lipid solubility o >99% unionized o t1/2ke0 2.6 minutes · Rapid offset by distribution: o ? due to similar factors o t1/2α fast 2 mins · Rapid metabolism: o Cl 30-60mL/kg/min o Phase 1 (CYP) and phase 2 o No active metabolites |
|
RF ideal features |
· Rapid onset: o 20x more lipid soluble than morphine o 68% unionized cf. morphine 23% o t1/2ke0 1.4 mins (cf. morphine 7) · Rapid offset by metabolism: o Cl 40mL/kg/min o Non-specific esterases especially muscle o Max context sensitive half time (CSHT) 10 mins o No active metabolites |
|
Lack of interference |
· No competition for plasma protein binding sites o PPF albumin o RF: AAG > albumin · No competition for metabolic pathways o PPF liver CYP2B6/2C9/3A4 o RF non-specific esterases · No competition for excretion (renal for both) |
|
Implications of synergism |
· ↓Ce for given clinical effect · ↓Infusion rate · ↓total dose · ↓compartmental concentrations · ↓time to emergence |
Pharmaceutics:
|
Precipitation |
No |
|
Miscible |
No (need separate syringes) |
Indications for TIVA:
|
Medical |
· Malignant hyperthermia (absolute indication) · ↑ ICP (PPF decreases CMRO2 and CBF, but preserves coupling ratio) · PHx PONV (PPF 5HT3 antagonist hence antiemetic; cf. volatiles pro-emetic) · Avoid paralysis (e.g. muscular dystrophy (RF -> ETT tolerance) · Sinus surgery (PPF ↓mAP -> ↓bleeding) |
|
Logistical |
· Airway surgery precluding volatile use (absolute indication) · Field anaesthesia · Transport |
Feedback welcome at ketaminenightmares@gmail.com