2020A15 Discuss the effects of ageing on the respiratory system.
List:
· Summary
· Upper airway
· Mechanics
· Volumes
· Gas exchange
· Control of breathing
Summary:
|
Changes |
· Degeneration of tissues · Progressive functional impairment from ~35 years |
|
Implications |
· Reduced reserve · Poor tolerance of stress (e.g. exercise, post-laparotomy) · Susceptible to types 1 and 2 failure |
Upper airway:
|
Musculature |
· ↓Pharyngeal dilator muscle tone -> ↑risk OSA |
|
Reflexes |
· ↓Airway reflexes -> ↓clearance of secretions -> ↑risk aspiration |
Mechanics:
|
Airway resistance |
· Senile emphysema -> ↓radial traction -> ↑dynamic compression in forced expiration -> ↓PEFR, ↓FEV1 |
|
Lung compliance |
· Senile emphysema -> ↓elastic recoil -> ↑risk of breath stacking during mechanical ventilation |
|
Chest wall compliance |
· ↓Compliance -> ↓outward recoil -> ↑work of breathing: due to o Calcification of costal cartilage o Joint degeneration o Barrel shape -> flattened diaphragm -> mechanical disadvantage o Osteoporosis -> kyphosis, ↑A-P diameter |
|
Musculature |
· Sarcopaenia (type II > type I) -> ↓PEFR, ↓FEV1, ↓MVV |
|
Breathing pattern |
· Small ↑airflow resistance · Large ↓resp system compliance · Hence ↑RR, ↓TV but ↔MV for a given lean mass |
Volumes:
|
Volumes |
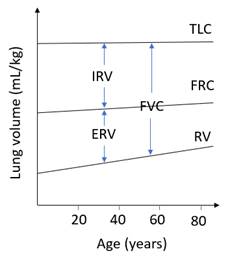
· Senile emphysema -> o ↑↑RV (~1%/year), ↑FRC (~0.2%/year) o ↓FVC (~0.5%/year), ↓ERV · Complex effect on TLC; minimal change overall o ↑Lung compliance -> ↑TLC o ↓Chest wall compliance -> ↓TLC o Atrophy of intervertebral discs -> ↓thoracic height -> ↓TLC o Altered geometry -> hyperinflation -> ↑TLC
|
|
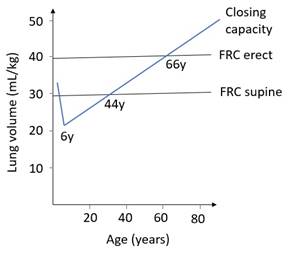
Closing capacity |
· Senile emphysema -> ↓airway splinting in expiration o ↑closing capacity -> ↑shunt -> ↓PaO2 § Present when standing § Worse when standing
|
Gas exchange:
|
Ventilation |
· Senile emphysema -> ↓radial traction -> small airway closure -> ↓PaO2 · Sarcopaenia -> ↓MVV |
|
Perfusion |
· ↓Cardiac output -> ↓O2 transfer (perfusion-limited in health) |
|
Matching |
· Widening of V&Q scatter from apex to base -> impaired gas exchange o ↑Alveolar dead space (but ↔PaCO2) o ↑Shunt (with ↓PaO2) |
|
Diffusion |
· ↑Alveolar thickness (fibrosis) · ↓Alveolar surface area (senile emphysema) ->
↓DLCO (0.2mL/mmHg/year) |
|
Overall |
·
↓O2 transfer + ↓max cardiac
output + sarcopaenia-> ↓VO2max |
Control of breathing:
|
Chemoreceptors |
· Dysfunction of central and peripheral receptors |
|
Respiratory centre |
· ↑Periodic breathing · ↓↓Response to ↓PaO2 and ↑PaCO2 · ↑Toxicity of opioids |
Feedback welcome at ketaminenightmares@gmail.com