2016B02 Compare and contrast the actional potentials from the sino-atrial node and a ventricular myocyte.
List:
· Intro
· Graphs and conductances
· Pacemaker action potential
· Ventricular myocyte action potential
Intro:
|
· Allows rapid, co-ordinated signalling · Rapid depolarisation followed by repolarization · Ion channels cycle through resting -> activated -> inactivated states |
|
|
Determinants of ion flux |
· Channel permeability: voltage dependent · Electrochemical gradients o Na+ and Ca2+ into cell, K+ out of cell o Mainly due to Na+K+ATPase |
Graphs and conductances:
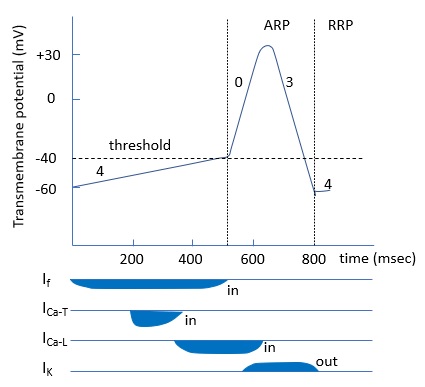
Pacemaker action potential:
|
Features |
· Automaticity o i.e. intrinsic, rhythmic, frequent depolaristion and contraction o HCN channel produces ‘funny current’ – i.e. mixed Na+ and K+ influx o [cAMP] ∝ If ∝ slope of phase 4 ∝ heart rate o Note depth of repolarisation ∝ IK ∝ 1/(heart rate) · Post-repolarisation refractoriness o RRP extends into phase 4 |
|
Refractory periods |
· Effective (ERP): insufficient HCN and Ca2+ channels resting; action potential (AP) impossible · Relative (RRP): enough HCN and Ca2+ channels resting but fewer than normal; AP possible with higher than normal stimulus |
|
Factors increasing rate |
· ↑SNS -> ↑If = ↑ICa > IK -> ↑steepness all slopes, especially phase 4 · ↑Temp -> ↑cell metabolic rate (enzymes, pumps) · ↓K+ -> less hyperpolarisation · Neonate: ↑resting HR (fixed stroke volume) |
|
Factors decreasing rate |
· ↑PSNS: -> ↓If, ↑IK -> ↓steepness phase 4, increased hyperpolarisation · ↓Temp -> ↓cell metabolic rate (enzymes, pumps) · Hypoxia -> failure of Na+K+ATPase, unable to repolarize cell, HCN not reactivated · Elderly: fibrous/fatty change in conduction system, ↓β1 adrenoceptors |
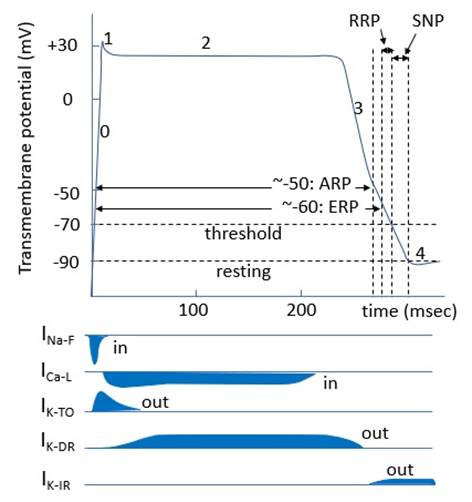
Ventricular myocyte action potential:
|
Features |
· Plateau -> time for systolic ejection and prevention of tetany · Variable timing -> co-ordinated contraction o e.g. endocardial cells start earlier, finish later |
|
Refractory periods |
· Absolute (ARP):no Na+ channels resting; AP impossible · Effective (ERP): insufficient Na+ channels resting; AP impossible · Relative (RRP): enough Na+ channels resting, but fewer than normal; AP possible with higher than normal stimulus
·
Supranormal period (SNP): AP possible with lower
than normal stimulus |
|
Autonomic changes |
· SNS: ↓ duration of action potential (phosphorylation of phospholamban -> ↑Ca2+ reuptake) |
|
Pathological changes |
· Hypoxia: failure of Na+K+ATPase -> depolarisation to -50mV -> inactivation of fast-Na+ channel and activation of L-Ca2+ channel -> behaves like pacemaker cell -> arrhythmia |
Feedback welcome at ketaminenightmares@gmail.com