2020B01 a)
Describe the immediate cardiovascular responses to the sudden loss of 30% blood
volume in a healthy awake person.
b) How are these responses different if the patient is undergoing anaesthesia
with sevoflurane?
List:
· Intro
· Status awake
· Status with sevoflurane anaesthesia
· Other responses
Intro:
|
Quantification |
· 30% blood loss (~1500mL) = Class 3 shock · Severe, life-threatening |
|
If awake |
· Immediate neural response · Later hormonal and rheologic responses |
|
If anaesthetised |
· All responses attenuated · High risk of decompensation and death |
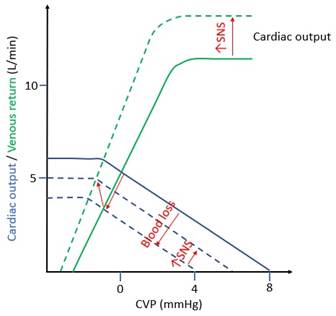
Effects of 30% blood loss:
|
Graph |
VR = (MSFP – RAP) / RVR VR: venous return MSFP: mean systemic filling pressure RAP: right atrial pressure RVR: resistance to venous return |
|
Direct effect |
· ↓↓MSFP -> ↓VR · ↓Cardiac output · ↓mAP · ↓Tissue perfusion |
|
Baroreceptor response |
à ↑CO, ↑SVR, ↑mAP Afferent limb: · Stretch-activated mechanoreceptors on C fibre visceral afferents · ↓Stretch -> ↑output to medulla and hypothalamus · Arterial pressure: carotid and aortic sinuses · Blood volume: receptors in atria and great veins Efferent limb: · ↑SNS output from rostral ventrolateral medulla · ↓PSNS output from vagal centres · ↑ADH release · ↓ANP release |
|
Blood reservoir mobilisation |
à ↑Blood volume ~500mL -> ↑MSFP · Source: spleen red pulp, liver sinusoids, skin arterioles / venules / A-V anastomoses · Mechanism: ↑SNS output -> α1 -> vasoconstriction |
|
Interstitial fluid reabsorption |
à ↑Blood volume -> ↑MSFP · Mechanism: ↑SNS output -> constriction of pre-capillary sphincters -> ↓capillary hydrostatic pressure -> net fluid reabsorption |
|
Restlessness |
à ↑MSFP, ↑venous return · ↑SNS -> ↑skeletal muscle pump activity |
|
Central ischaemic response |
à ↑CO, ↑SVR, ↑mAP · CNS hypoperfusion -> ↑↑SNS output · For redirection of flow to vital organs in extremis |
|
Endocrine response |
(minutes to hours) · ↑ADH -> ↑H2O reabsorption from collecting duct -> water preservation · ↑RAAS -> ↑Na+/H2O reabsorption -> ECF preservation |
|
Rheologic response |
(days to weeks) · ↑Epo -> ↑erythropoiesis -> restoration of red cell mass |
If anaesthetized with sevoflurane:
|
Cellular effects |
· Inhibition of L-Ca2+ channels (heart and vasculature) · ↑Nitric oxide release (vasculature) · GABA potentiation -> ↓medullary SNS output (heart and vasculature) |
|
Physiological effects |
· ↓Contractility · Relative preservation of baroreceptor reflex -> ↑HR · Venodilatation -> ↓venous return, ↓preload · Vasodilatation -> ↓SVR, ↓afterload · ↓Cardiac output · ↓mAP |
|
Effects on shock |
Detrimental: · Direct effects exacerbated · All compensatory responses attenuated · Effects are dose-dependent Protective: · Relative preservation of baroreceptor reflex · ↑SNS output in Guedel’s stage 2 |
Other responses:
|
Decompensation |
· ↑↑SNS · ↑Metabolic rate (↑cardiac, respiratory, skeletal muscle work) · ↑Anaerobic metabolism · ↓pH · ↓inotropy, arrhythmia, death · Greatly increased risk under sevoflurane anaesthesia |
|
Ischaemic pre-conditioning |
· Brief ischaemic episode improves tolerance of subsequent episode · Mechanism: activation of sarcolemmal and mitochondrial K+-ATP channel · Mimicked by volatile anaesthesia (anaesthetic pre-conditioning) |
Feedback welcome at ketaminenightmares@gmail.com