2009A09 Discuss
the physiological factors that determine intracranial pressure (ICP).
Describe how changes in posture affect ICP.
List:
· Intro
· Monroe-Kellie doctrine
· Factors affecting each component
· Head down: effect and compensation
· Head up: effect and compensation
Introduction: ICP
|
Definition |
· Force per unit area within the cranial vault |
|
Normal |
· 5-10mmg in the supine position, measured at the external auditory meatus |
|
Determinants |
· a) intracranial volume (fixed) · b) amount of brain, blood and CSF |
Monroe-Kellie doctrine:
|
Description |
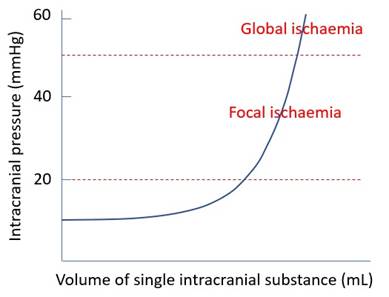
· Cranium has fixed walls and one major outlet · An increase in one substance must come at the expense of another, otherwise pressure rises rapidly |
|
Elastance curve |
|
|
Volume buffering |
· Venous blood -> circulation: rapid response, lower capacity · Arterial blood -> circulation: minimal · CSF cranial -> spinal: slower response, higher capacity |
Volume determinants:
|
Parenchyma (80-85%) |
· ↑Volume: oedema, tumour, abscess · ↓Volume: atrophy |
|
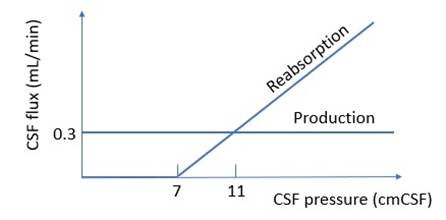
Cranial CSF (7-10%) |
N.B.: a) X axis unit mmCSF not mmHg b) Y axis zero point not at the X axis
· ↑Volume: obstruction to circulation, Trendelenburg · ↓Volume: CPP <70mmHg -> no production, reverse Trendelenburg |
|
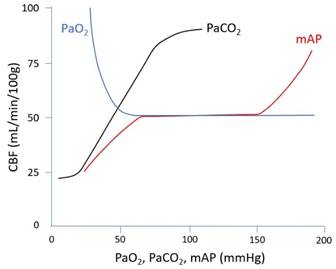
Blood (5-8%) |
· ↑Volume: o ↑Temp, seizure (↑CMRO2 -> vasodilatation) o ↑PaCO2 (↑[H+] in CSF and brain ECF -> vasodilatation) o ↓PaO2 (vasodilatation) o ↑↑mAP?* o Trendelenburg (↑venous pressure) o Neck strictures (↑venous pressure) · ↓Volume o ↓Temp o ↓PaCO2 o ↓↓mAP?* o Reverse Trendelenburg
(*The relationship between mAP and CBV is not clear to me) |
Trendelenburg:
|
Example |
· Gynae laparoscopy · Say -10mmHg = -13.5cm |
|
Direct effect |
· Add 10mmHg hydrostatic pressure · CNS arteries: 100 -> 110 mmHg (1.1x normal) -> small ↑arterial volume · CNS veins: 2-> 12mmHg (6x normal) -> large ↑venous volume |
|
Compensation |
· CSF displaced -> ↓CSF volume (compensation) · Parenchyma: no change |
|
Overall effect |
· Mild ↑ICP |
Erect:
|
Example |
· Shoulder surgery · Say +22mmHg = +30cm |
|
Direct effect |
· CNS arteries: 100 -> 78mmHg (0.8x normal) -> small ↓ volume · CNS veins: 2 -> -20mmHg (-10x normal) -> large ↓ volume · CSF: cranial to spinal -> ↓ volume · Parenchyma: unchanged |
|
Compensation |
· Myogenic response: ↓mAP -> ↓stretch -> reflex cerebral vasodilatation -> ↑CBV -> ↑ICP · Central ischaemic response: ↓↓mAP -> CNS acidosis -> ↑SNS output -> ↑HR, ↑SVR, ↑mAP (often reflex bradycardia i.e. Cushing response) |
|
Overall effect |
· ICP falls from +5mmHg to -10mmHg · CVP becomes the limiting factor for CPP (Starling resistor) |
Addit: means of reducing ICP:
|
Physical |
· Head up 30° (↓CVP) · Loosen any neck strictures (↓CVP) |
|
Physiological |
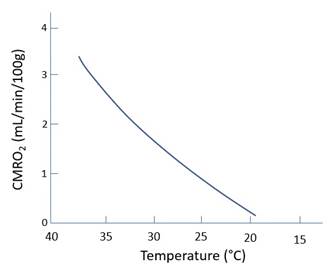
· ↑pO2 (normalise CBF) · ↓pCO2 (↓CBF · ↓Temp (↓CMRO2 -> ↓CBF) (note doesn’t improve outcomes after TBI) |
|
Pharmacological |
· Hypnotics: propofol, thiopentone (↓CMRO2) · Anti-epileptics: e.g. levetiracetam (↓CMRO2 if seizure) · Muscle relaxants: e.g. cisatracurium (↓coughing and Valsalva -> ↓CVP) · Osmotic agents: hypertonic saline, mannitol (↓parenchymal water) |
|
Psurgical |
· External ventricular drain (↓CSF) · Decompressive craniectomy (note doesn’t improve outcomes after TBI) |
Feedback welcome at ketaminenightmares@gmail.com