2015B05 Describe how morbid
obesity affects time to awakening (not wash-out)
after inhalational anaesthesia.
List:
· Morbid obesity
· Emergence modelling
· Final end-tidal partial pressure
· Elimination from V1
· MAC-awake
Morbid obesity:
|
Definition |
· BMI >35kg/m2 body surface area |
|
Changes |
· ↑Lean mass (20% of excess) -> ↑BMR, ↑cardiac output, ↑VA · ↑Fat mass (80% of excess), cephalad diaphragm displacement, ↓FRC · Inflammatory cytokines -> ↓MAC |
|
Overall effects on time to emergence (TTE) |
· Short case: ↑distribution rate -> ↓time to emergence (TTE)
·
Long case: ↑uptake ->
↑TTE · Washout of drug is invariably slower |
|
Implications |
· Prefer desflurane -> ↓accumulation (mainly due to lean mass) · Prefer adjuvants -> ↓MAC -> ↓accumulation |
Emergence modelling:
|
Determinants of TTE |
1. Final partial pressure in effect site prior to washout 2. Rate of elimination from V1 3. Partial pressure in V1 associated with emergence (MAC-awake) |
|
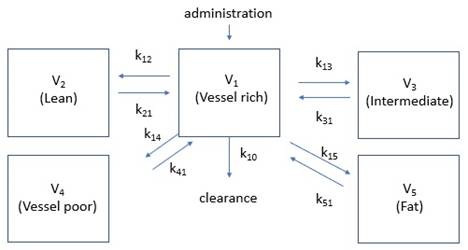
Kinetic model |
Equilibration time constants: · τ= 1/k · τ= (V x λ) / Q · (V = volume of tissue, λ = tissue: blood partition coefficient, Q = blood flow) Significant effects of MO: · ↑Cardiac output but tissue blood flow per unit mass · ↑V2, V3 -> ↑TTE after moderate duration case · ↑↑V5 -> ↑TTE after long duration case |
|
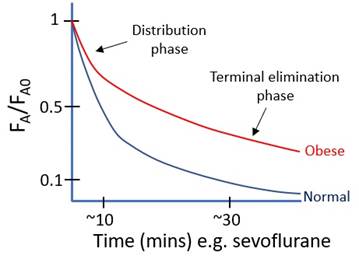
Washout curve |
|
|
Putative effect site |
· Ascending reticular activating system, thalamus frontal cortex · Concentration correlates with that in V1 · May not be included in kinetic model · Rate of equilibration between effect site and VRG ∝ o Blood flow to brain per unit mass (not % cardiac output to brain) o 1/(brain-blood partition coefficient) |
1.Final end-tidal partial pressure: (factors decreasing it)
|
Infusion |
· ↓Duration (MO: difficult surgery) · ↓Inspired % (MO: ↑uptake hence ↑inspired % for given expired %) |
|
Drug |
· ↑Tissue:blood partition coefficients (MO ↑ as above) o ↑Muscle:blood PC (sevo 3.1, des 2.0, iso 2.9) o ↑Fat:blood PC (sevo 48, des 27, iso 45) · ↓MAC (MO: cytokines -> ↓) o Correlates with ↓oil:gas PC (sevo 80, des 29, iso 98) · ↑Metabolism (MO: +/- liver disease -> ↓) |
|
Patient |
· ↑Cardiac output (MO ↑) · ↑Tissue volumes (MO ↑) |
2.Elimination from V1: (factors accelerating it)
|
Short case |
Offset during distribution phase: · ↑Cardiac output (MO ↑) · ↑Tissue:blood PC (MO ↑) · ↑Compartment volumes (MO ↑) |
|
Long case |
Offset during terminal elimination phase: · ↓Cardiac output (MO ↑) · ↓Tissue:blood PC (MO ↑ · ↓Compartment volumes (MO ↑) · ↑Metabolism (MO: +-/ liver disease -> ↓) · ↑Excretion (MO: complex effect on VA:FRC ratio) o ↑metabolic rate -> ↑VCO2 -> ↑awake ventilation; but o ↓Chest wall compliance -> ↓ventilation under GA
o
↓Chest wall compliance ->
↓↓FRC under GA and supine; |
3.MAC awake: (normal ~0.33)
|
Patient factors |
· ? Adipokines -> ↓MAC-awake · ? Sleep-disordered breathing -> ↑narcotic sensitivity -> ↓MAC-awake |
Feedback welcome at ketaminenightmares@gmail.com