2018B05 Describe the maternal cardiovascular changes that occur during pregnancy.
List:
· Summary
· Haemodynamics
· Blood
· Regional circulation
· Labour
· Other
Summary:
|
Objectives |
· Support foetal gas exchange · Prepare for massive PPH |
|
Most important changes |
· ↑Blood volume · ↑Interstitial volume · ↑Cardiac output · ↑Coagulability |
|
Causes |
· Placental hormones · ↑Demand |
Haemodynamics:
|
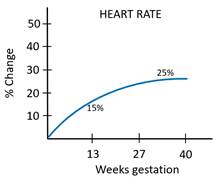
Heart rate |
· ↑Uteroplacental demand -> ↑venous return (Note: ↑HR occurs from ~4/40, not conception) |
|
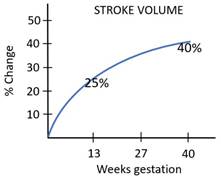
Stroke volume |
· ↑Uteroplacental demand -> ↑venous return · ↑RR and VT -> ↑respiratory pump (Note: ↑SV occurs a bit later than for heart rate) |
|
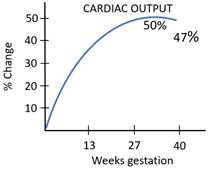
Cardiac output |
· ↑Uteroplacental demand · Note increased risk of heart failure |
|
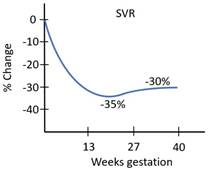
Systemic vascular resistance |
· Progesterone, prostaglandins -> · Smooth muscle relaxation · Downregulation of α1 adrenoceptors |
|
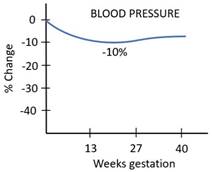
Blood pressure |
· ↓↓Diastolic, ↓systolic, ↑pulse pressure · Due to ↓SVR with ↑stroke volume |
Blood:
|
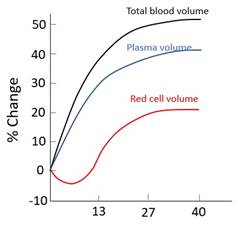
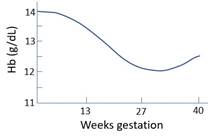
Blood volume |
· Causes: o Oestrogen -> ↑RAAS -> retain Na+, H2O o Oestrogen -> ↑Epo · Implications: o Iron supplementation aids erythropoiesis o Hypervolaemic haemodilution improves tolerance of massive PPH o Hypoviscosity aids increased cardiac output |
|
Interstitial volume |
· Mucosal swelling, peripheral oedema · Causes: o Oestrogen -> ↑RAAS o Progesterone -> vasodilatation · Implication: o ? Fluid reserve in case of blood loss (no evidence for this) |
|
Plasma proteins |
· ↓[Albumin], ↔AAG · ↓Oncotic pressure 14% · Cause: progesterone -> volume expansion -> dilution · Implication: ↑free % acidic drugs e.g. ↑risk thiopentone toxicity if GA LUSCS |
|
Hypercoagulability |
· ↑Factors I (2x), VII, VIII, IX, X, XII, vWF · ↓Protein S, acquired resistance to Prot C · Cause: oestrogen · Implication: ↓risk lethal bleeding, ↑risk thromboembolism |
Regional circulations:
|
Uterine blood flow |
· 150mL/min -> 750mL/min (80% uteroplacental, 20% other) · Cause: ↑demand · Implication: potential for rapid bleeding |
|
Other |
· Renal blood flow: ↑80%, mostly in T1 o Hence ↑urine output · ↑Flow rate through skin, muscle, breast, GIT o Hence faster onset of SC and IM drugs (e.g. opioid in labour) |
Labour:
|
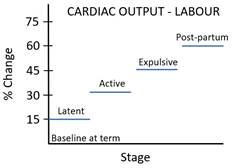
Escalating cardiac output |
· Intrapartum: effort + pain + distress (attenuated by epidural) · Post-partum: uterine involution -> autotransfusion (highest risk of heart failure) |
Pathology:
|
Supine aortocaval compression |
· i.e. supine -> ↓↓mAP · Blood shunted to azygos systems · Affects 15% patients · From 20/40 · Prevention: wedge under right hip during LUSCS or resuscitation |
|
Pre-eclampsia |
· Cause: ? abnormal invasion or spiral arteries by trophoblast · Characterised by multi-system endothelial dysfunction · Risk of hypertensive emergency and seizure |