1999A04 Explain
how the kidney handles glucose. Describe the physiological
consequences of glycosuria.
List:
· Renal handling
· Consequences of glycosuria
Renal handling:
|
Filtration |
· Polar but small molecule 180g/mol · Freely filtered · Normal plasma concentration 4mM, hence 900mM/day |
|
Reabsorption |
· Near 100% · From urine into cell: o Via sodium-glucose cotransporter-1 (SGLT1) in proximal straight tubule o Via SGLT2 in proximal convoluted tubule o Gradient established by basolateral Na+K+ATPase o i.e. secondary active transport · From cell into interstitium: o Via GLUT-2 (i.e. facilitated diffusion) · Water follows by osmosis |
|
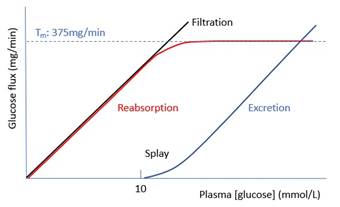
Graph |
· Transport maximum (TM): o Due to limited number and capacity of SGLT2 · Splay: due to differential reabsorptive capacity of nephrons o Predicted threshold: 375/125/180 = 0.0167M = 16.7mM o Actual threshold: 10mM · Effect of SGLT-2 inhibitor: (my thoughts only!) o Downward shift of TM o Hence leftward shift of excretion curve |
Consequences of glycosuria:
|
Renal |
· ↑Tubular and urinary [glucose] · Osmotic diuresis · Washout of hypertonic medullary interstitium · ↑Na+/K+ antiport in distal nephron · ↑Risk UTI |
|
Systemic |
· Dehydration, ↑osmolality · ↓blood volume, ↓mAP, ↓organ perfusion, ↓pH, organ dysfunction · Loss of nutrient and energy · Loss of Na+: due to medullary washout · Loss of K+: due to medullary washout and ↑Na+/K+ antiport in distal nephron (aldosterone) |
|
Compensatory responses |
· To hyperosmolality: ↑ADH · To hypovolaemia: ↑ADH, ↓ANP · To hypotension: ↑SNS, ↑RAAS, ↑ADH |