2011B15 Outline the physiological changes that might explain why an
otherwise well patient
may have a reduced urine output intra-operatively.
List:
· Intro
· Glomerular filtration physiology
· Factors decreasing filtration
· Factors increasing reabsorption
Intro:
|
Urine output determinants |
= filtration + secretion – reabsorption |
|
Normal urine output |
0.5mL/kg/h |
|
Peri-op effects |
↓filtration: hypotension ↑Reabsorption: stress response, dehydration Hence ↓urine output |
Glomerular filtration physiology:
|
Starling equation |
GFR = [K(Pc – PB) – σ(πc – πB)] · Pc (capillary hydrostatic pressure) is the major variable peri-operatively · Dependent on a) renal blood flow b) afferent and efferent arteriolar tone |
|
Renal blood flow |
RBF = mAP – CVP / renal vascular resistance (RVR) · Myogenic autoregulation effective if mAP 70-170mmHg |
|
Mean arterial pressure |
mAP – CVP = CO x TPR · Factors ↑CO: ↑preload, ↓afterload, ↑rate, ↑contractility |
Factors decreasing filtration:
|
↓mAP |
↓Cardiac output · ↓preload (general or neuraxial anaesthesia, IPPV, dehydration) · ↓inotropy (e.g. propofol) ↓SVR: · General anaesthesia · Neuraxial anaesthesia |
|
↑CVP |
· IPPV · Heart failure · Raised intra-abdominal pressure |
|
↑RVR |
Angiotensin 2 (AGTR1) and SNS (α1) -> efferent > afferent arteriolar constriction |
Factors increasing reabsorption:
|
↑ADH |
Source: hypothalamus -> posterior pituitary Release stimuli: · Stress response from surgery · Many drugs · ↑osmolality (sensitive to ∆2%) – dehydration from pre-op fasting · ↓blood volume (sensitive to ∆10% but overrides osmolality) · ↓mAP · Angiotensin 2 Renal effects: · Insertion of aquaporin 2 into apical membrane of collecting ducts -> ↑H2O reabsorption · Insertion of urea transporters -> ↑ medullary interstitial osmolarity · ↑Na+ reabsorption in thick ascending loop of Henle |
|
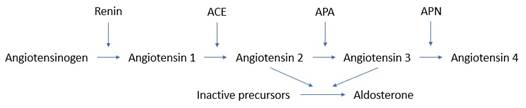
↑RAAS |
Source: granular cell of juxtaglomerular apparatus Release stimuli: · ↑SNS activation of granular cells (β1) - e.g. pain · ↓stretch of afferent arteriolar baroreceptors - i.e. hypotension · ↓NaCl delivery to macula densa -> ↑PGE2, ↓adenosine release - i.e. ↓GFR Renal effects of angiotensin 2 · ↑Na+/H2O reabsorption from PT (via Na+/H+ exchange) (AGTR1) · ↑release of aldosterone · ↑release of ADH Actions of angiotensin-3: · 40% of pressor activity · 100% of aldosterone induction Renal effects of aldosterone · ↑Na+ reabsorption from principal cells of connecting tubule and collecting ducts (MR) · Indirectly causes H2O reabsorption via ↑ECF osmolality hence ↑ADH |
|
↑SNS |
Stimulus: baroreceptor reflex Renal effects: · Constrict efferent > afferent arterioles(α1) · Hence ↓GFR but preserved GFP · ↑ proximal tubular reabsorption of Na+/H2O (α1) · ↑ renin release (see RAAS) (β1) |