2012B10 Outline the mechanisms by which the kidney maintains potassium homeostasis.
List:
· Intro
· Filtration
· Reabsorption
· Secretion
Intro:
|
Normal values |
· ECF 3.5-5mM (tight control required for cell function) · ICF 150mM · Intake 1-1.5mmol/kg/day · Output: urine >> faeces, sweat |
|
Renal potassium handling |
· Freely filtered · Fixed fraction reabsorbed (~95%) · Variable secretion · Small amount compulsory excretion (5%) |
|
Significance |
· Lower priority than sodium reabsorption · Compulsory excretion means compulsory intake ~0.5mmol/kg/day |
Filtration:
|
Freely filtered |
· 180L/day x 4mM = 720mmol/day |
|
Minimal variation |
· Minimal variation in ECF concentration · Minimal variation in GFR: autoregulation to 125mL/min o Myogenic: ↓afferent arteriolar stretch -> reflex dilatation (effective for mAP 70-170mmHg) o Chemical (tubuloglomular feedback): ↓NaCl at distal tubule -> reflex dilatation o Hormonal (renin-angiotensin): ↓afferent arteriolar stretch or ↓NaCl at distal tubule -> ↑renin |
Reabsorption:
|
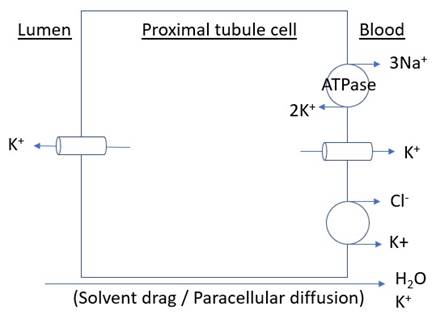
Proximal tubule (65%) |
· Paracellular transit: o Solvent drag o Passive diffusion
|
|
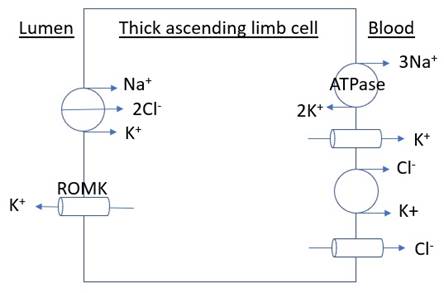
Loop of Henle (~20%) |
· Secondary active transport (major) · Passive paracellular diffusion (minor)
|
|
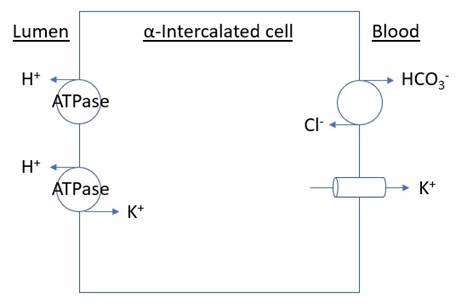
Collecting ducts (~10%) |
(alpha intercalated cell) · Active transport
|
Secretion:
|
Location |
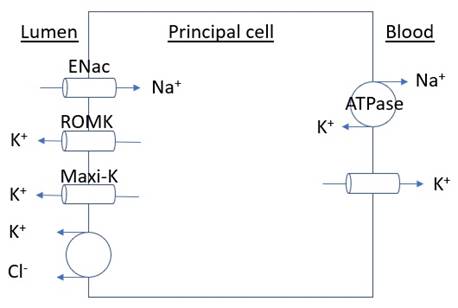
· Principal cell of the connecting tubule and collecting duct |
|
Mechanism |
· Secondary active transport
|
|
Effect of aldosterone |
· Stimuli for release: o CRH -> ACTH (necessary for synthesis; minor stimulus for release) o Angiotensin 2 (major) o Hyperkalaemia (minor) · Effect on principal cell o ↑Na+K+ATPase synthesis and activity o ↑ENaC and ROMK activity o i.e. ↑Na+ reabsorption at expense of ↑K+ secretion |
|
Other physiology |
Factors increasing K+ secretion: · ↑ECF [K+] (↑Na+K+ATPase activity independent of aldosterone) · ↑Urine or Na+ flow rate (e.g. glycosuria) · ↑Non-Cl- anions |
|
Drugs |
· Loop diuretics: inhibit Na+K+2Cl- symporter, hence ↑tubular flow, ↑K+ secretion · Thiazide: inhibit Na+Cl- reabsorption in distal convoluted tubule -> ↑tubular flow, ↑K+ secretion · MR antagonist: ↓Na+K+ATPase synthesis and activity, ↓ROMK activity -> ↓K+ secretion |
|
Pathology |
· Renal failure: ↓GFR -> ↓tubular flow -> ↓K+ secretion -> risk hyperkalaemia |

Recommended reading: https://cjasn.asnjournals.org/content/10/6/1050.full