2005B09 Describe
the gravity-dependent processes which affect pulmonary blood flow.
What changes take place when the pressure increases in the pulmonary vessels?
List:
· West zones: erect
· West zones: other positions
· Effect of increased pulmonary vascular pressures
West zones: erect
|
Summary |
· Gravity creates a hydrostatic pressure gradient: base > apex · Lung divided into regions according to relationship between alveolar, vascular and interstitial pressures |
|
Z1 |
· PA > Pa > Pv · Minimal apical lung in health · = Alveolar dead space · No blood flow (Q) · ↑Z1 if o ↑PA: e.g. IPPV, PEEP o ↓Pa: e.g. pulmonary embolus, haemorrhage, ↓inotropy, pulmonary vasodilator) |
|
Z2 |
· Pa > PA > Pv · From 3cm above RV to near apex in health · Starling resistor: o Diastole: Pa<PA hence Q = 0 and downstream Pv irrelevant o Systole: Q begins when Pa >> PA; then Q ∝ (Pa-Pv) o (↑↑ pressure required to re-open collapsed vessel) |
|
Z3 |
· Pa > Pv > PA · From near base to 3cm above RV · Majority of lung tissue · Q continuous. |
|
Z4 |
· Pa > Pi > Pv > PA · Q minimal? · Compression of extra-alveolar vessels: o Base of lung at low volume in health (↓ radial traction) o APO (↑ interstitial fluid) |
West zones: other positions
|
Summary |
· Hydrostatic pressure gradient ∝ vertical height of lung · Erect > lateral decubitus > supine |
|
Lateral decubitus |
· Z1: almost zero lateral non-dependent lung · Z2: almost whole non-dependent lug · Z3: almost dependent lung · Improved V/Q matching c.f. supine |
|
Supine |
· Z1: minimal anterior both lungs · Z2: minimal mid-anterior both lungs · Z3: most of both lungs · No right-left inequality |
|
Prone |
· More even distribution o Gravity favours flow in non-dependent areas o Lung architecture favours flow in dependent areas |
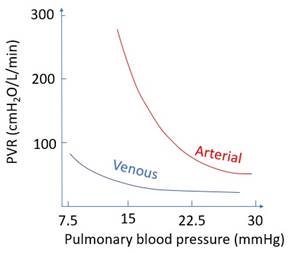
Effect of increased pulmonary vascular pressures:
|
Effect |
· ↑PAP or ↑PVP -> ↓ PVR · Unlike systemic circulation |
|
Purpose |
· Allows high flow rate without high pressure (e.g. exercise) · Minimises transdation hence diffusion distance · Hence preserves gas exchange |
|
Mechanisms |
· Recruitment: ↑ pressure -> re-open collapsed vessels (Z1) · Distension: ↑pressure -> ↑ radius of open vessels (Z2,3) · ↑Vascular surface area -> ↓PVR o Q = (P1-P2)/R o R = (8 x length x viscosity) / (π x radius4) assuming laminar |
|
Graph |
|
Unrelated: effect of prone positioning on ventilation and perfusion
|
|
Ventilation |
Perfusion |
|
Awake supine |
Better ventrally: · Dorsal diaphragm displaced cephalad o ↑Mechanical advantage · Dorsal lung compressed a bit by ventral lung/heart/abdo viscera o ↓Volume -> ↑compliance |
Better dorsally: · Lung architecture -> dorsal flow · Gravity -> dorsal flow |
|
GA supine |
· Dorsal diaphragm displaced a lot · But now akinetic · Dorsal lung compressed a lot -> small airway collapse, atelectasis, ↓compliance · (Worse if ARDS) |
Better dorsally (as above) |
|
GA prone |
More evenly spread · Lung/mediastinum/abdo viscera supported by sternum and ribs (not dorsal lung) · More homogeneity of intrapleural pressure / lung volume / lung compliance |
More evenly spread · Lung architecture -> dorsal flow · Gravity -> ventral flow |
(see Tobin, 1999 Anaesthesia and Intensive Care)