2016B01 Describe
the respiratory effects of adding positive end-expiratory pressure (PEEP) to intermittent
positive pressure ventilation (IPPV).
List:
· Intro
· Benefits
· Harm
· Clinical use
Intro:
|
Definition |
· Positive end-expiratory pressure |
|
Overall purpose |
· Counteract the fall in FRC that occurs with anaesthesia · Prevent collapse of small airways and alveoli o Especially dependent regions o Especially at extubation o Note recruitment manoeuvres are required to re-open collapsed areas |
|
Typical range |
· 5-15cmH2O |
Benefits of PEEP:
|
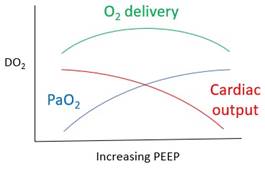
↑Oxygenation |
· ↑Lung volume -> ↑Alveolar surface area -> ↑gas exchange · Prevent collapse -> ↓shunt->↑PaO2 -> ↑DO2 · Note theoretical ‘sweet spot’ for DO2
(might not be so simple - see Nunn’s Applied Respiratory Physiology, Fig 30.3) |
|
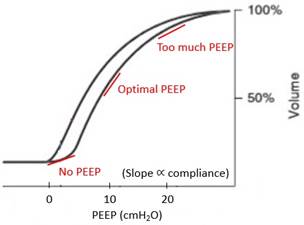
↑Lung compliance |
· ↑Static compliance: due to ↑lung volume -> ↑alveolar radius · ↑Dynamic compliance: due to prevention of small airway and alveolar collapse ->↓Airway pressure, ↓damage
(modified from West’s Respiratory Physiology) |
|
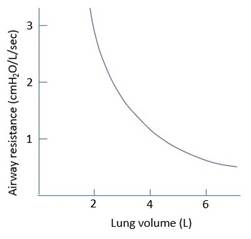
↓Airway resistance |
· Laminar flow: R = (8 x length x viscosity) / (π x radius4) · Turbulent flow: (P1-P2) ∝ (length x density) / (radius5) · PEEP -> ↑Lung volume -> ↑airway radius -> ↓resistance · Radius is the major factor, since power 4 or 5 ->↓Airway pressure, ↓damage
|
|
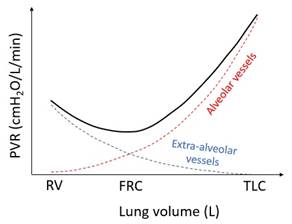
↓Pulmonary vascular resistance |
· Low volume: compress extra-alveolar vessels · High volume: compress alveolar vessels -> PVR minimized at natural FRC
|
|
Prevent damage |
· ↓Alveolar collapse, ↓atelectrauma -> ↓Shear stress -> ↓Inflammation |
Harm from PEEP:
|
Alveolar damage |
· Over-PEEP -> barotrauma, volutrauma, pneumothorax, pneumomediastinum |
|
Breath stacking |
· ↓Expiration rate -> stacking -> trauma · Higher risk if asthma, COPD |
|
Dead space |
· ↑Alveolar pressure -> ↑West zone 1 |
|
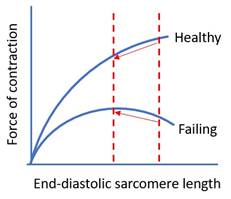
Impede cardiac output |
· ↑Intrathoracic pressure -> obstruction to venous return · Higher risk if hypovolaemia |
Clinical use:
|
General anaesthesia |
· Prevent ↓FRC, with all the above benefits |
|
Acute cardiogenic pulmonary oedema (as CPAP) |
· Obstruction of venous return -> normalization of preload · ↓Transmural pressure- > ↓afterload · Move alveolar water into interstitium · Increases lymphatic drainage · (No effect on total lung water)
|
|
Type 2 respiratory failure (as BiPAP) |
· Splints airways during expiration -> shift equal pressure point proximally -> ↓airway collapse -> ↓obstruction |