2018A13 Define and describe LUNG compliance. Describe the difference between static and dynamic compliance.
List:
· Graphs x 2
· Static compliance
· Determinants of static compliance
· Dynamic compliance
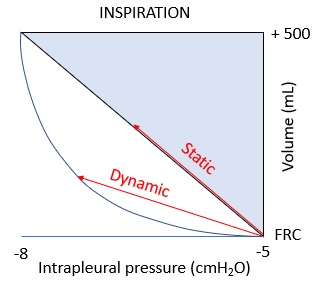
· Difference between static and dynamic compliance: i.e. hysteresis
· Causes of hysteresis: airflow resistance, time-dependence
Graphs:
Static compliance
|
Definition |
· ∆volume/∆transpulmonary pressure (TPP) when airflow has stopped |
|
Normal |
· 200mL/cmH2O |
|
Measurement in spontaneous ventilation |
· Inhale known volume from FRC, pause with open glottis · Distal oesophageal manometer for intrathoracic pressure ≈ intrapleural pressure · ∆P = distal oesophageal pressure – mouth pressure · (Pmouth ≈ Palveolus) |
|
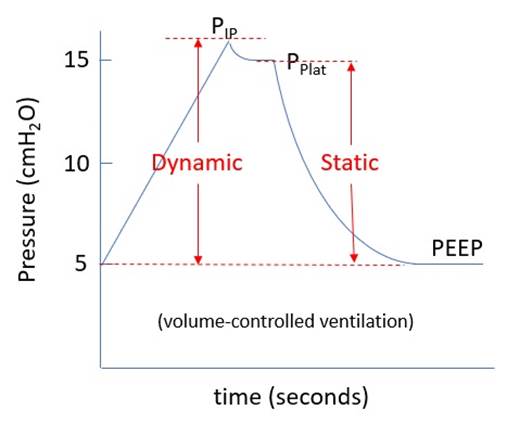
Measurement in mechanical ventilation |
· Volume control ventilation (fixed inspiratory flow rate) · ∆P = Plateau pressure – PEEP |
Determinants of static compliance:
|
· Elderly/smoking -> emphysema -> ↓inward recoil -> ↑LC · Fibrosis -> ↓LC · Pulmonary oedema -> ↓LC |
|
|
Surfactant |
· LaPlace’s law: Pressure (P) = 2 x surface tension (T) / radius (r) o Fluid surfaces acquire least surface area due to surface tension o Alveoli tend to collapse · Role of surfacant o Amphipathic molecule o Reduces surface tension at air-water interface o Becomes more concentrated (= more effective) at low alveolar volume o -> ↓alveolar collapse, ↑compliance · Factors increasing surface tension: o Alveolar oedema -> surfactant dilution · Surfactant deficiency (e.g. prematurity, SP-B or SP-C deficiency) |
|
Absolute lung size |
· Reasons: o ↑Alveolar number -> ↑LC o ↑Alveolar size -> ↑LC (↑radius -> ↓pressure – LaPlace) · Examples: o Adult > Neonate (100 cf. 1.5-6mL/cmH2O) o Male > Female o Tall > Short · N.B. compliance constant if indexed to size (i.e. compliance/FRC) |
|
Relative lung volume |
· High: surfactant spread out -> ↑ST -> ↓ LC · Low: ↓ radius -> ↑ST, alveolar collapse -> ↓LC o e.g. pregnancy, obesity · Max compliance at FRC |
|
Gravity |
· Basal compression -> ↓alveolar volume at FRC -> ↑basal LC · Apical traction -> ↑alveolar volume at FRC -> ↓apical LC |
|
Posture |
· Supine: ↓LC o Dorsal lung compressed by ventral lung/mediastinum/abdo viscera o Awake: compression + -> dorsal LC > ventral LC o Under GA: compression +++ -> ventral LC > dorsal LC · Prone: ↑LC o Lung/mediastinum/abdo viscera supported by sternum and ribs o ↑Uniformity of intrapleural pressure / volume / compliance · Overall ↑FRC and ↑LC (esp. if abdomen free) |
|
Pulmonary blood volume |
· Congestion -> ↓ LC · (e.g. heart failure, supine posture) |
Dynamic compliance (DC):
|
Definition |
· ∆volume/∆transpulmonary pressure during airflow |
|
Normal |
· 50-100mL/cmH2O · i.e. much less than static compliance |
|
Measurement in spontaneous ventilation |
· Cannot measure directly · Pmouth ≠ Palveolar due to airway resistance |
|
Measurement in mechanical ventilation |
· Volume controlled ventilation · ∆V/(peak inspiratory pressure – PEEP) |
Difference between static and dynamic compliance: i.e. hysteresis
|
Definition |
· The lag in a property of a system behind changes in the factor determining that property |
|
Manifestations |
· Lung volume lags behind changes in airway pressure · For a given lung volume, TPP during inspiration > TPP during expiration |
Causes of hysteresis:
Resistance to airflow:
|
Equations |
· Laminar: R = (8 x length x viscosity) / (π x radius4) · Turbulent: (P1-P2) ∝ length x density / radius5 |
|
Determinants: |
↑Resistance if: ·
↓Airway radius o ↓Absolute lung size (e.g. neonate cf. adult) o Relative lung volume (e.g. diaphragm displacement in pregnancy) o Intraluminal obstruction (e.g. mucus) o Luminal obstruction (bronchoconstriction, swelling) o Extraluminal obstruction (e.g. dynamic airways compression) · ↑Viscosity: e.g. ↑temp · ↑Length |
Time-dependence:
|
1) Surfactant changes |
· Lag in even spread -> lag in equilibration of surface tension between alveoli · For a given lung volume: surface tension in inspiration > surface tension in expiration · *most important factor* |
|
2) Stress relaxation |
· Due to viscoelasticity of collagen |
|
3) Pendelluft |
· Distribution of air from fast-τ to slow- τ lung units at end inspiration and early expiration · τ= resistance x compliance · Fast unit: low resistance, low compliance · Slow unit: high resistance, high compliance · e.g. bronchoconstriction -> ↑resistance -> ↑τ |
|
4) Recruitment |
· Recruitment of collapsed alveoli during inspiration · Quasi Starling resistor · e.g. collapse after thoracic surgery |
Feedback welcome at ketaminenightmares@gmail.com