2021A15 Describe the respiratory responses to hypoxaemia in both the awake and the anaesthetized patient.
List:
· Intro and importance
· Hyperventilation: sensor, integrator, effector
· Hypoxic pulmonary vasoconstriction
· Sympathetic outflow
Intro: hypoxaemia
|
Definition |
· PaO2 < 60mmHg |
|
Responses |
· Increased alveolar ventilation -> ↑PaO2 · Hypoxic pulmonary vasoconstriction o Improved V/Q matching -> ↑PaO2 o ↑PVR · ↑SNS output -> ↑cardiac output -> DO2 |
|
Effect of anaesthesia on responses |
· Suppression of all responses · Dose-dependent effects |
|
High risk if: |
· Alone (e.g. post-op ward at night) · CO2-insensate (e.g. severe COPD, OSA, OHS) · Sensitive to resp depression (e.g. elderly, neonate) · Respiratory depressant drugs (e.g. morphine) · Sedated (e.g. midazolam) · Synergistic respiratory depressant drugs (e.g. benzo+ opioid) |
Alveolar hyperventilation:
Sensor:
|
Structure |
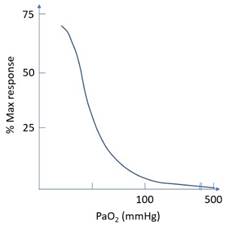
· Peripheral chemoreceptors o Carotid bodies (CNIX Hering’s nerve) o Aortic bodies (CNX) · Type 1 glomus cell: responsive to ↓pO2, ↑pCO2, (↓pH carotids only) · Type 2 sustentacular cell: support · Blood flow 2000mL/min/100g -> supply by dissolved O2 only |
|
Function |
· ↓ PaO2 -> closure of K+ channel -> depolarisation -> ↑afferent to resp centre · Response is minimal until PaO2 <100mmHg, profound <50mmHg · Response is rapid, <1 second
|
|
Effect of anaesthesia |
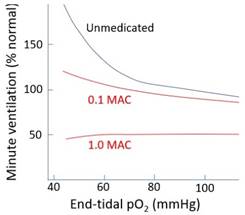
· Volatiles: o ↓Chemoreceptor afferents is the most important resp effect o 1 MAC: ablated response o 0.1 MAC: significant depression of response o Hence need for O2 supplementation post-op for safety
· Propofol: o ↓Chemoreceptor afferents o Less potent than volatiles |
Controller:
|
Structure |
· Respiratory centre, medulla · Multiple cell types: dorsal inspiratory, ventral expiratory, pre-Botzinger pacemakers · Afferents via nucleus tractus solitarius · Efferents via nucleus ambiguus and dorsal motor nucleus of CNX |
|
Function |
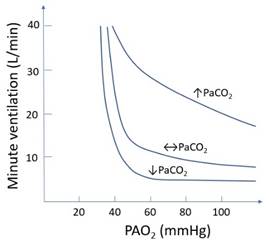
· ↑Stimulation -> ↑amplitude and frequency of neuronal output to effectors · ↓PaO2 is synergistic with ↑PaCO2 and ↓pH
|
|
Effect of anaesthesia |
· Suppression: o General anaesthesia (↑GABA/glycine activity) o Opioids (μ receptor agonist in resp centre – most important opioid effect) o Neuraxial: ↓input to reticular activating system -> ↓conscious state, ↓resp centre output · Stimulation: o Pain -> ↑input to reticular activating system -> ↑resp centre output |
Effector:
|
Muscles |
· Primary inspiratory: diaphragm, external intercostals, pharyngeal dilators · Accessory inspiratory: e.g. sternocleidomastoid · Expiratory: e.g. internal intercostals, abdominals (normally inactive) |
|
Function |
· ↑Respiratory centre output -> ↑RR, VT -> ↑VA -> ↑PaO2 · Completion of negative feedback loop |
|
Effect of anaesthesia |
· Volatile: o Skeletal muscle relaxation (inhibit nAChR) o Inhibit a-motor neuron (↑GABA/↑glycine) o Affects intercostals > diaphragm · Propofol: o As for volatiles o But less potent: ↓glycine activity, ↓spinal cord effect · Benzodiazepines: o Skeletal muscle relaxation · Neuraxial: o Inhibit α-motor neuron (intercostals) o No effect on diaphragm unless C-spine level · Paralysis: o No effector response · Position: o Supine, Trendelenburg -> ↑work of breathing -> impaired effector · Apparatus dead space (tubing distal to Y piece): o ↓VA for a given MV |
Hypoxic pulmonary vasoconstriction:
|
Aim |
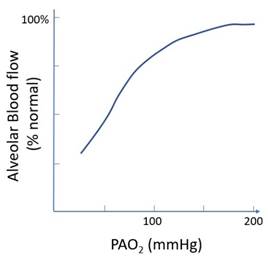
· Match ventilation with perfusion, ↑PaO2 |
|
Mechanism |
· Vasoconstriction ∝ 1 / (PAO20.6 x PvO20.4) |
|
Biphasic response |
· Phase 1: onset immediate, plateau 5 mins o ? Inhibition of K+ channel o ? ↓mitochondrial ROS o ? ↓ATP:ADP · Phase 2: onset 40 minutes, plateau 2 hours o ? ↑↓COX, LOX production o ? ↑hypoxia-inducible transcription
|
|
Effect of anaesthesia |
· Volatile: o Inhibit L-Ca2+ channel, ↑NO release, ↓medulla SNS output o Generalised vasodilatation including pulmonary · Propofol: o Similar mechanisms o Less potent, preferred in one lung ventilation |
Sympathetic response:
|
Stimulus |
· ↓PaO2 <50mmHg -> CNS acidosis |
|
Response |
· ↑SNS output · ↑HR, ↑contractility, venoconstriction -> ↑preload · ↑Cardiac output -> ↑O2 delivery · No change to PaO2 |
|
Effect of anaesthesia |
· Volatiles, propofol: o ↓SNS output from medulla (↑GABA, glycine activity) o Inhibit L-Ca2+ on heart, blood vessels o ↑Nitric oxide release o Dose-dependent suppression of baroreceptor response (propofol > volatiles) · Opioids, benzodiazepines: o ↓SNS output · Neuraxial: o ↓SNS output below block upper limit |
Feedback welcome at ketaminenightmares@gmail.com