2021B10 Discuss possible causes for the PaCO2 differing from the ETCO2 in an anaesthetised, intubated patient on IPPV.
Intro:
|
Normal |
· Gap in health 2-5mmHg (PaCO2 > etCO2) · Due to alveolar, anatomical and apparatus dead space |
|
Causes |
1. Dead space 2. Incomplete alveolar emptying 3. Measurement error 4. Sampling error |
1.Dead space:
|
Definition |
· That portion of the tidal volume that does not undergo gas exchange |
|
Components |
· Apparatus dead space (distal to Y piece) · Physiological dead space o Anatomical dead space (conducting airways) o Alveolar dead space (non-perfused alveoli) |
|
Pathophysiology |
· Ideal alveolus: PACO2 = PaCO2 ≈40mmHg · Dead space: PACO2 ≈ 0.4mmHg · End-tidal air is a mix of both, hence etCO2 < PaCO2 |
|
Measurement |
Physiological: · Bohr equation: VD/VT = (PACO2 – PECO2) / PACO2 o If PA = ideal alveolar gas -> measure of anatomical dead space o If PA = end-expiratory gas -> measure of physiological dead space · Enghoff modification: substitute PaCO2 for PACO2 o Measure of physiological dead space o Assumes stable cardiac output o
Assumes PaCO2 = (ideal) PACO2
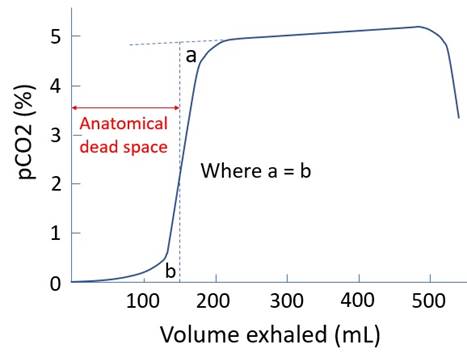
Anatomical: · Estimated by Fowler’s method · Volume of gas exhaled before pCO2 reaches a plateau · Normal 2mL/kg
Alveolar: · VD = physiological - anatomical · Minimal if healthy and conscious
Apparatus: · Estimable using product information
|
|
Alveolar DS |
a.k.a. West Zone 1: · PA > Pa > Pv · hence vascular collapse · Small volume near apices in health when upright ↑PA if: · IPPV (∝ airway pressure) ↓Pa if: · Pulmonary vasodilators (e.g. milrinone) · Negative inotropes (e.g. propofol) · Reduced venous return (e.g. hypovolaemia) Effect of GA: · ↔Non-ventilated alveoli · ↑Hypoventilated alveoli (due to maldistribution of V and Q) |
|
Anatomical DS |
Cause of absolute increase: · ↑Tidal volume (plateau at VT ~350mL) · Bronchodilation (sevoflurane, pregnancy) Cause of absolute decrease: · ↓↓Tidal volume o Axial streaming o Cardiac impulse -> mixing (Note ↓VT increases relative dead space) · LMA or ETT (bypasses upper airway) |
|
Apparatus DS |
· Device and tubing distal to Y junction · Important in small children · ETT/LMA: VD is 1/2 of VT · Face mask: VD is 2/3 of VT |
2.Incomplete alveolar emptying:
|
Causes |
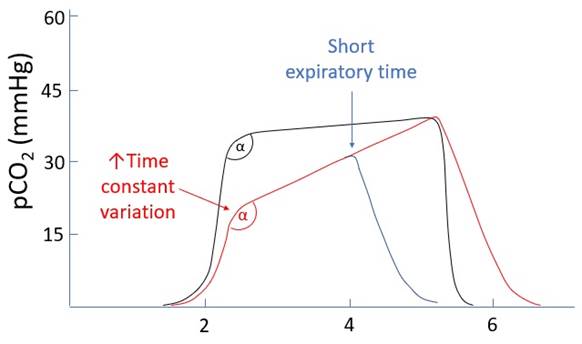
· ↑Variation in time constants (e.g. asthma, COPD) · ↓Expiratory time (↑RR, ↓IE ratio) · (especially if both are present) |
|
↑Variation in time constants |
· Time constant (τ) = resistance x compliance · Slow lung units: ↑R,↑C o Slow rate of change o ↓Ventilation o ↑pCO2 Empties late in expiration · Fast lungs units: ↓R,↓C o Fast rate of change o ↑Ventilation o ↓pCO2 Empties early in expiration · Hence variation -> ↑α angle
|
3.Measurement error:
|
Confusion |
· N2O 4.5μm, CO 4.7μM (causes falsely high pCO2) · H2O vapour absorbs widely (causes falsely high pCO2) · Inhaler propellant and halothane · FIX: reference chamber AND water trap |
|
Collision broadening |
· Widening of the absorption peak for one gas in the presence of another · Due to collision between molecules raising their energy level · 50% N2O widens CO2’s absorption peak by 10% · FIX: use reference chambers |
|
Ram-gas effect |
· Pressure-drop across the sampling line · ↓ total pressure inside sample chamber -> ↓ CO2 partial pressure |
|
Calibration failure |
· FIX: auto regular three point calibration |
4.Sampling error:
|
Dilution by FGF |
· Sampling of FGF may occur in expiration if high RR and low VT · e.g. neonates and young children |
|
Disconnection |
· Complete disconnection: ambient air · Partial disconnection: entrainment of some room air |
|
Blockage |
· By water condensation |
Feedback welcome at ketaminenightmares@gmail.com